Vernal keratitis, a severe form of vernal keratoconjunctivitis (VKC), represents the corneal involvement in this chronic, recurrent ocular allergic condition. Predominantly affecting children and adolescents, especially males in hot and arid climates, this disease can result in substantial visual impairment if left untreated. It is marked by persistent inflammation of the conjunctiva and cornea, leading to epithelial damage, shield ulcers, and potential vision loss.

Epidemiology and Risk Profile
- Age Group: Common in children aged 5–15 years.
- Gender: Higher prevalence in males (approx. 2:1 ratio).
- Geographical Distribution: Most frequent in Africa, the Middle East, South Asia, and Central/South America due to warm, dry climates.
- Seasonality: Peak symptoms in spring and summer.
Pathogenesis and Immune Response
Vernal keratitis is driven by a complex immunological reaction involving both IgE-mediated and T-cell–mediated hypersensitivity responses. Mast cells, eosinophils, and Th2 cytokines are major contributors to the chronic allergic inflammation observed in the conjunctiva and cornea.
Clinical Features of Vernal Keratitis
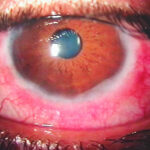
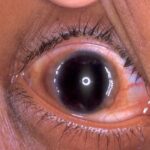
Vernal keratitis manifests with both conjunctival and corneal symptoms. The hallmark of corneal involvement is the development of shield ulcers and punctate epithelial keratitis, which can threaten vision.
Ocular Symptoms
- Severe ocular itching
- Burning sensation and tearing
- Photophobia (light sensitivity)
- Foreign body sensation
- Thick mucoid discharge
- Pain in case of ulceration
Corneal Signs
1. Shield Ulcers
A pathognomonic feature of vernal keratitis. These are shallow, sterile ulcers with a grayish-white base, primarily located in the upper cornea due to mechanical abrasion by giant papillae on the upper tarsus.
- Grade 1: Transparent base with no inflammatory material
- Grade 2: Opaque base with fibrinous plaque
- Grade 3: Hard plaque not removable without debridement
2. Punctate Keratitis
Fine, superficial epithelial erosions usually seen in early VKC cases.
3. Corneal Neovascularization
Chronic inflammation may lead to peripheral corneal vascularization.
Subtypes of Vernal Keratoconjunctivitis Associated with Keratitis
1. Palpebral VKC
Marked by giant cobblestone papillae on the upper tarsal conjunctiva. Corneal damage occurs due to mechanical trauma from these enlarged papillae.
2. Limbal VKC
Characterized by gelatinous hypertrophy of the limbal conjunctiva and presence of Horner-Trantas dots—accumulations of eosinophils and epithelial cells.
3. Mixed VKC
Involves both palpebral and limbal manifestations, often indicating a more aggressive disease course.
Diagnostic Workup
Clinical Examination
- Slit-lamp Biomicroscopy: Essential to assess papillae, limbal changes, corneal ulcers.
- Fluorescein Staining: Highlights corneal epithelial defects and ulcer margins.
Cytological Analysis
- Conjunctival scrapings reveal eosinophils, confirming allergic etiology.
Differential Diagnosis
- Herpes simplex keratitis
- Atopic keratoconjunctivitis
- Bacterial keratitis
- Mooren’s ulcer
Treatment Strategies for Vernal Keratitis
Prompt treatment is crucial to prevent complications such as scarring and vision loss. The therapeutic approach includes symptom control, inflammation suppression, and corneal healing promotion.
Environmental Control
- Minimize exposure to allergens, dust, wind, and bright sunlight.
- Use protective eyewear and cold compresses.
Medical Management
1. Antihistamines and Mast Cell Stabilizers
- Olopatadine, ketotifen, azelastine, and epinastine provide dual action in controlling allergic inflammation.
- Long-term mast cell stabilizers like nedocromil or lodoxamide help reduce recurrence.
2. Topical Steroids
Effective for acute exacerbations, particularly in severe corneal involvement.
- Preferred options: Loteprednol, fluorometholone (low risk of IOP elevation)
- Short-duration usage under ophthalmic supervision is critical to minimize risks.
3. Topical Immunomodulators
- Cyclosporine A 0.05%–0.1%: Reduces steroid dependence and controls chronic inflammation.
- Tacrolimus 0.03% ointment: Especially useful in steroid-resistant cases.
4. Management of Shield Ulcers
- Debridement of ulcer base in Grade 2–3 ulcers.
- Topical antibiotics to prevent secondary infection.
- Lubricating eye drops to support epithelial healing.
- Bandage contact lenses (BCLs) to promote re-epithelialization and relieve symptoms.
Surgical Options
Indicated in severe cases unresponsive to medical treatment.
- Amniotic membrane transplantation
- Papillae excision
- Superficial keratectomy
Prognosis
With timely and effective intervention, most patients experience remission of symptoms by late adolescence. However, untreated or recurrent cases with persistent keratitis may develop:
- Corneal scarring
- Visual acuity reduction
- Irregular astigmatism
- Steroid-induced glaucoma or cataract
Preventive Measures
- Early diagnosis and seasonal prophylaxis
- Routine ophthalmologic evaluations
- Judicious use of corticosteroids
- Education on allergen avoidance
- Avoidance of eye rubbing to prevent trauma and exacerbate inflammation
Vernal keratitis is a serious manifestation of VKC that requires vigilant clinical attention due to its potential to impair vision. A multidisciplinary treatment strategy—encompassing anti-allergic agents, immunomodulators, and surgical care when necessary—offers optimal outcomes. Ensuring early intervention, continuous monitoring, and allergen control are pivotal in preventing long-term sequelae and preserving visual function in affected children and adolescents.