Streptococcus pyogenes, also known as Group A Streptococcus (GAS), is a gram-positive, beta-hemolytic bacterium responsible for a spectrum of infections. Among these, traumatic skin lesion S. pyogenes infections are particularly concerning due to the organism’s aggressive nature and potential to invade deep tissues.
Following skin trauma — including lacerations, abrasions, puncture wounds, or surgical incisions — the breached epidermal barrier provides an entry point for colonization. When not promptly recognized and treated, the infection can evolve into cellulitis, erysipelas, or necrotizing fasciitis, each requiring urgent intervention.
Pathogenesis of Streptococcus pyogenes Infection in Skin Trauma
Mechanism of Infection Initiation
- Breach in Skin Integrity: Traumatic injuries expose subdermal tissues.
- Bacterial Invasion: S. pyogenes adheres via surface proteins (e.g., M protein, fibronectin-binding proteins).
- Toxin Production: The pathogen releases exotoxins such as streptolysins, hyaluronidase, and streptococcal pyrogenic exotoxins, promoting tissue destruction and immune evasion.
- Systemic Spread: Invasive strains may enter the bloodstream, causing bacteremia, toxic shock syndrome, or sepsis.
Clinical Presentation and Diagnosis
Common Signs and Symptoms
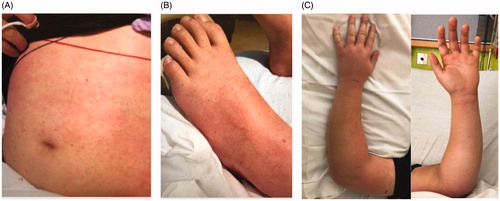
- Localized Erythema and Swelling: Typically within 24–48 hours of trauma.
- Pain Out of Proportion: A hallmark of invasive infections such as necrotizing fasciitis.
- Purulent or Serosanguinous Discharge
- Fever, Malaise, Lymphadenopathy
- Rapidly Expanding Lesion with Induration
Diagnostic Evaluation
- Physical Examination: Assessment of lesion depth, progression, and systemic signs.
- Laboratory Studies:
- CBC with elevated leukocytes
- CRP and ESR often markedly increased
- Blood cultures in systemic symptoms
- Microbiological Confirmation:
- Wound swab or aspirate culture identifying β-hemolytic, catalase-negative, bacitracin-sensitive S. pyogenes
- Imaging: MRI or ultrasound to evaluate for abscess or deep tissue involvement
Risk Factors and Susceptible Populations
Factors Increasing Susceptibility
- Recent Trauma or Surgery
- Compromised Skin Integrity: Burns, ulcers, insect bites
- Chronic Illnesses: Diabetes mellitus, peripheral vascular disease
- Immunosuppression: HIV, chemotherapy, corticosteroid use
- Poor Hygiene or Contaminated Environments
Differential Diagnosis
When evaluating a traumatic skin lesion for potential S. pyogenes infection, consider alternative or co-infective pathogens:
- Staphylococcus aureus (including MRSA)
- Pseudomonas aeruginosa (especially in burn wounds)
- Clostridium spp. (gas gangrene in necrotic wounds)
Timely differentiation is essential for effective antimicrobial selection and treatment strategy.
Treatment of Streptococcus pyogenes Skin Infections
Antibiotic Therapy
- First-line:
- Penicillin G or V (IV for systemic infections; PO for mild cases)
- Severe or Necrotizing Cases:
- Penicillin + Clindamycin to inhibit toxin production
- Allergy to Penicillin:
- Cephalosporins, or macrolides (e.g., azithromycin)
Surgical Intervention
- Debridement: Essential in necrotizing fasciitis to remove infected tissue.
- Drainage: For abscess or localized pus collections.
Supportive Measures
- IV fluids for hemodynamic stability
- Antipyretics and analgesics
- Intensive monitoring for systemic complications
Prevention and Infection Control
Wound Management Protocols
- Immediate Cleansing of Wounds: Use sterile saline or antiseptic solutions.
- Avoid Occlusive Dressings that trap moisture unless indicated for healing.
- Tetanus Prophylaxis in trauma with uncertain immunization status.
Prophylactic Antibiotics
- Reserved for high-risk wounds (deep punctures, contaminated injuries, immunocompromised patients)
Infection Surveillance
- Educate patients and caregivers on early warning signs: redness, increasing pain, warmth, or pus formation.
- Routine follow-up for post-trauma wound care in clinical settings.
Complications of Untreated Infections
- Necrotizing Fasciitis
- Sepsis and Toxic Shock Syndrome
- Endocarditis
- Post-streptococcal glomerulonephritis
Timely diagnosis and intervention are crucial to mitigate life-threatening complications.
Public Health and Epidemiological Considerations
Community-Acquired vs Nosocomial Infections
Most S. pyogenes skin infections are community-acquired, often linked to trauma in sports, overcrowded living conditions, or poor wound hygiene.
Outbreak Control
- Isolate infected individuals in communal settings
- Disinfect shared items and surfaces
- Promote hygiene education and handwashing campaigns
Future Directions in Management
- Rapid PCR-Based Diagnostics: Enhanced accuracy in early detection
- Vaccines Under Development: Targeting M protein epitopes
- Antimicrobial Stewardship Programs: Reducing resistance development through judicious antibiotic use
Frequently Asked Questions:
What is the most common symptom of S. pyogenes skin infection?
Redness, swelling, and rapidly worsening pain at the site of trauma are typical early symptoms.
How soon after injury can infection develop?
Symptoms usually appear within 24 to 48 hours post-injury.
Can these infections become life-threatening?
Yes, especially if they progress to necrotizing fasciitis or systemic sepsis.
Is S. pyogenes contagious?
Yes, it can spread through direct contact with infected wounds or contaminated objects.
Can antibiotics alone treat invasive infections?
In severe cases like necrotizing fasciitis, antibiotics must be combined with surgical debridement.
Traumatic skin lesion Streptococcus pyogenes infections represent a serious clinical challenge with potentially life-threatening outcomes. Through rapid recognition, accurate diagnosis, and comprehensive treatment — including targeted antibiotics, surgical management, and preventive care — we can effectively control and mitigate the impact of this aggressive pathogen. Vigilant wound care, patient education, and public health initiatives remain essential pillars in preventing recurrence and community spread.