Tertiary syphilis is the most severe and potentially life-threatening stage of syphilis, a chronic bacterial infection caused by Treponema pallidum. Occurring years or even decades after the initial untreated infection, this phase is marked by irreversible damage to vital organs, including the heart, brain, skin, and bones. While rare in developed nations due to early diagnosis and antibiotic access, tertiary syphilis still presents a significant clinical concern in areas with limited healthcare.
Disease Progression: From Infection to Tertiary Stage
The progression of syphilis is typically divided into four stages: primary, secondary, latent, and tertiary. Without treatment, approximately 15–30% of infected individuals may develop tertiary syphilis.
Pathophysiology of Tertiary Syphilis
In the tertiary stage, T. pallidum triggers a granulomatous inflammatory response that affects multiple systems. The bacteria are often difficult to detect directly, and damage results largely from immune-mediated processes.
Key Manifestations:
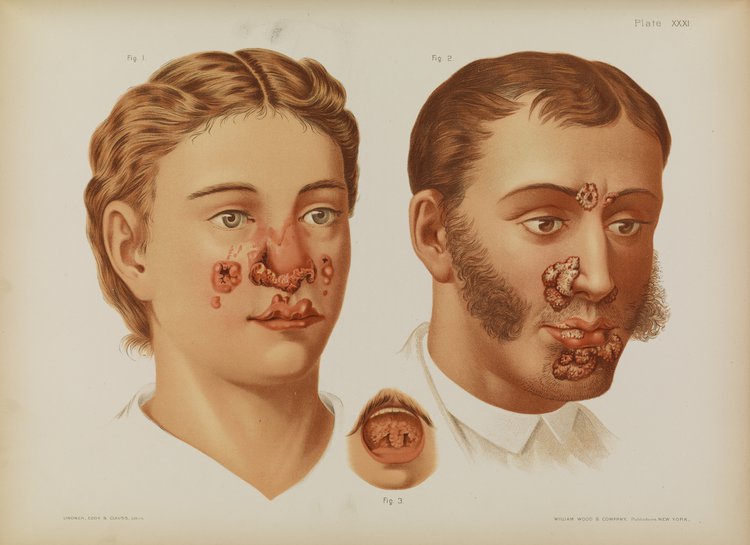
- Gummatous Syphilis: Granuloma-like soft tissue lesions
- Cardiovascular Syphilis: Aortitis and aortic aneurysms
- Neurosyphilis: Tabes dorsalis, general paresis, dementia
Gummatous Syphilis
Gummas are chronic, destructive lesions that may affect skin, bones, and internal organs.
Characteristics:
- Painless, rubbery nodules
- Can ulcerate and cause tissue destruction
- Common sites: skin, liver, bones
Gummatous lesions typically appear 3–10 years after the initial infection and may mimic malignancies or other granulomatous diseases.
Cardiovascular Syphilis
Cardiovascular complications generally arise 10–30 years after infection.
Key Findings:
- Syphilitic Aortitis: Inflammation of the ascending aorta
- Aortic Aneurysm: Risk of rupture and sudden death
- Aortic Valve Regurgitation: Leads to heart failure symptoms
- Coronary Ostial Stenosis: Reduced myocardial perfusion
This form is often asymptomatic until catastrophic complications develop.
Neurosyphilis
While neurosyphilis may appear at any stage, tertiary neurosyphilis is defined by slow, progressive degeneration of neurological function.
Clinical Forms:
- Tabes Dorsalis: Demyelination of the dorsal columns and sensory nerves
- Lightning pains
- Ataxia
- Urinary incontinence
- Argyll Robertson pupils
- General Paresis: Cognitive decline, personality changes, dementia
- Meningovascular Neurosyphilis: Stroke-like syndromes due to vasculitis
Diagnosis of Tertiary Syphilis
Given the long latency and complex manifestations, a comprehensive diagnostic approach is essential.
Serological Testing:
- Non-Treponemal Tests: VDRL, RPR
- Quantitative; used to monitor treatment response
- Treponemal Tests: FTA-ABS, TPPA
- Qualitative; remain positive for life
CSF Analysis (For Neurosyphilis):
- Elevated protein and WBC
- Positive CSF-VDRL confirms diagnosis
Imaging:
- MRI or CT: Brain and spinal cord evaluation
- Echocardiogram: Aortic valve and aneurysm detection
- X-ray/Bone Scan: Gummatous involvement in bone
Differential Diagnosis
| Condition | Overlapping Features | Key Differentiators |
|---|---|---|
| Tuberculosis | Chronic granulomas | Acid-fast bacilli, pulmonary involvement |
| Leprosy | Skin and nerve lesions | Peripheral nerve thickening, skin smear |
| Vasculitis (e.g., PAN) | Neurological and cardiac issues | Negative serology for syphilis |
| Autoimmune Encephalitis | Cognitive decline | Autoantibodies, MRI findings |
Treatment of Tertiary Syphilis
Standard Regimen:
- Benzathine Penicillin G 2.4 million units IM weekly for 3 weeks
For neurosyphilis:
- Aqueous crystalline penicillin G 18–24 million units/day, IV every 4 hours for 10–14 days
Alternative (For Penicillin Allergy):
- Desensitization is recommended due to penicillin’s superior efficacy.
- Doxycycline or Ceftriaxone may be considered but are less preferred.
Prognosis and Complications
With Treatment:
- Progression halted
- Some symptoms may partially reverse (e.g., early neurosyphilis)
Without Treatment:
- Progressive neurological deterioration
- Aortic rupture or heart failure
- Severe physical and psychological disability
Early detection and management remain critical to preventing irreversible organ damage.
Prevention and Public Health Considerations
Primary Prevention:
- Safe sexual practices (condom use)
- Routine STI screening in high-risk groups
- Partner notification and treatment
Secondary Prevention:
- Early detection through antenatal screening
- Prompt treatment of latent syphilis
Tertiary Prevention:
- Managing chronic complications
- Neurological rehabilitation
- Cardiovascular surgery when indicated
Frequently Asked Questions:
What is the difference between tertiary and latent syphilis?
Latent syphilis is asymptomatic, while tertiary syphilis causes organ damage and serious complications.
Can tertiary syphilis be cured?
The infection can be eradicated, but tissue damage is often permanent.
How long does it take to develop tertiary syphilis?
It usually develops 10–30 years after initial infection if left untreated.
Is tertiary syphilis contagious?
No, tertiary syphilis is not contagious. Infectiousness occurs only in the earlier stages.
What is the most serious form of tertiary syphilis?
Neurosyphilis and cardiovascular syphilis pose the greatest risks for disability and death.
Tertiary syphilis remains a medical challenge due to its complexity, delayed onset, and potentially devastating consequences. While modern antibiotics have rendered it largely preventable and curable, the importance of early diagnosis, public awareness, and continuous surveillance cannot be overstated. Addressing the burden of syphilis, particularly in underserved populations, remains a global public health imperative.

