Schizoaffective disorder (SAD) is a complex psychiatric condition that combines elements of schizophrenia and mood disorders such as bipolar disorder or depression. It is marked by psychotic symptoms, including hallucinations and delusions, alongside significant mood disturbances. One of the most concerning aspects of schizoaffective disorder is the heightened risk of suicidal behavior among affected individuals. Understanding the underlying causes, recognizing risk factors, and implementing effective treatment strategies are crucial in mitigating these risks and improving patient outcomes.
This article delves into suicidal behavior in schizoaffective disorder, providing an in-depth exploration of its symptoms, contributing factors, diagnostic approaches, and evidence-based management strategies.

Understanding Schizoaffective Disorder and Its Link to Suicidal Behavior
Schizoaffective disorder is characterized by both psychotic features (delusions, hallucinations) and mood disturbances (either depressive or manic episodes). These features can vary in severity, leading to significant functional impairment and emotional distress for individuals with the condition. Suicidal behavior in schizoaffective disorder is often associated with the intensity of both the psychotic symptoms and the mood disturbances.
What is Schizoaffective Disorder?
Schizoaffective disorder is a psychiatric diagnosis that presents a unique combination of symptoms typically seen in schizophrenia and mood disorders. It can be classified into two primary subtypes based on the mood component:
- Bipolar Type: Includes manic or mixed episodes alongside psychotic symptoms.
- Depressive Type: Involves depressive episodes along with psychosis.
The complex interplay between mood and psychotic symptoms is a significant factor in the occurrence of suicidal behavior in patients with schizoaffective disorder.
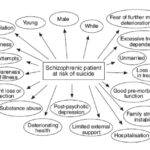
Suicidal Behavior: Risk Factors in Schizoaffective Disorder
Suicidal ideation and behavior are unfortunately common in individuals with schizoaffective disorder, with studies indicating that up to 30-50% of patients with SAD may attempt suicide at some point in their lives. Identifying the risk factors that contribute to suicidal behavior is critical in managing these patients effectively.
1. Psychotic Symptoms and Impaired Reality Testing
The psychotic symptoms of schizoaffective disorder, such as delusions and hallucinations, can lead to distorted thinking and perception of reality. This can cause intense emotional distress and feelings of hopelessness or despair. Individuals who experience persecutory delusions or command hallucinations may be at an elevated risk of suicide due to feelings of paranoia or commands to harm themselves.
2. Mood Disturbances: Depression and Mania
The presence of mood symptoms, particularly depression, significantly increases the risk of suicidal behavior in schizoaffective disorder. Depressive episodes often lead to feelings of worthlessness, isolation, and an inability to cope with stress, which can trigger suicidal thoughts. Conversely, manic episodes may also elevate suicide risk, especially when they involve impulsivity, poor judgment, or risky behavior.
3. Comorbidities: Substance Abuse and Personality Disorders
Patients with schizoaffective disorder often have comorbid conditions such as substance abuse, anxiety disorders, or personality disorders. Substance abuse, in particular, increases impulsivity and may impair judgment, making it more difficult for patients to engage in rational decision-making. The presence of a personality disorder, such as borderline personality disorder, can exacerbate feelings of emotional dysregulation, further increasing the likelihood of suicidal behavior.
4. Prior Suicide Attempts
A history of previous suicide attempts is one of the strongest indicators of future suicide risk. Individuals with schizoaffective disorder who have attempted suicide in the past may have a higher likelihood of future attempts, especially if their condition remains untreated or poorly managed.
5. Family History of Mental Illness or Suicide
Genetic factors play a role in the risk of suicidal behavior. A family history of mental health disorders or suicide can increase the susceptibility to suicidal ideation in individuals with schizoaffective disorder. These genetic predispositions can interact with environmental stressors, further heightening the risk.
Recognizing the Symptoms of Suicidal Behavior in Schizoaffective Disorder
Early detection of suicidal ideation is essential to prevent tragedy and reduce the long-term impact on patients and their families. Identifying the signs of suicidal behavior and taking prompt action can make a significant difference in outcomes.
Common Symptoms of Suicidal Behavior
- Verbal Expressions of Suicidal Thoughts: Patients may express thoughts of death, self-harm, or hopelessness, either directly or indirectly.
- Social Withdrawal: Isolation and detachment from friends, family, or social activities can signal a deterioration in emotional well-being.
- Mood Changes: Rapid mood swings, irritability, or profound sadness can be indicative of underlying depression or emotional distress.
- Neglect of Personal Care: A noticeable decline in personal hygiene or an inability to care for oneself may suggest a worsening mental state.
- Increased Substance Use: Escalating use of alcohol or drugs can reflect an attempt to numb emotional pain, and may increase the risk of impulsive suicidal actions.
Importance of Mental Health Screenings
Routine mental health screenings, including regular assessments for suicidal ideation, should be a part of the care plan for individuals with schizoaffective disorder. Screening tools, such as the Columbia-Suicide Severity Rating Scale (C-SSRS), can be invaluable in identifying at-risk individuals and facilitating timely intervention.
Treatment and Management of Suicidal Behavior in Schizoaffective Disorder
The management of suicidal behavior in schizoaffective disorder involves a multifaceted approach, combining pharmacological treatment, psychotherapy, and ongoing support. The goal is not only to alleviate the symptoms of schizoaffective disorder but also to address the specific factors contributing to suicidal behavior.
1. Pharmacological Treatment
Pharmacotherapy plays a crucial role in the treatment of schizoaffective disorder, particularly in managing both the psychotic symptoms and mood disturbances. Medications prescribed may include:
- Antipsychotics: To manage psychotic symptoms, such as delusions and hallucinations.
- Mood Stabilizers: Such as lithium or anticonvulsants, to control manic episodes and mood swings.
- Antidepressants: These are often used to address the depressive component of schizoaffective disorder.
- mTOR Inhibitors: In some cases, medications like mTOR inhibitors are considered for treating mood disorders associated with psychosis.
2. Psychotherapy and Counseling
Psychotherapy is a key component of treatment, particularly cognitive-behavioral therapy (CBT), which can help patients address negative thought patterns and develop healthier coping strategies. Dialectical behavior therapy (DBT) is also beneficial for individuals with emotional dysregulation, helping them manage impulsive behavior and emotions.
3. Crisis Intervention and Suicide Prevention Programs
For individuals at immediate risk of self-harm, crisis intervention strategies are critical. These may involve inpatient care, close monitoring, and the implementation of suicide prevention protocols. Support groups and community resources are also important for providing ongoing support and reducing feelings of isolation.
4. Long-Term Management and Follow-Up Care
Long-term management includes regular follow-up care to monitor the patient’s progress and adjust the treatment plan as needed. Continued therapy, medication management, and social support are essential in preventing relapse and reducing the risk of future suicidal behavior.
Improving Outcomes for Patients with Schizoaffective Disorder
Suicidal behavior in schizoaffective disorder is a serious concern that requires comprehensive and individualized treatment. Through a combination of pharmacological intervention, psychotherapy, and close monitoring, it is possible to reduce the risk of suicide and improve quality of life for patients with this condition. Early intervention, education for families, and ongoing support play crucial roles in managing the condition and preventing suicidal outcomes.