Squamous cell carcinoma of the head and neck (HNSCC) is a group of biologically similar cancers originating from the squamous epithelium lining the oral cavity, oropharynx, hypopharynx, and larynx. These malignancies represent over 90% of head and neck cancers and are most commonly associated with risk factors such as tobacco use, alcohol consumption, and human papillomavirus (HPV) infection.
Overview of Squamous Cell Carcinoma in Head and Neck
Squamous cell carcinoma develops from the flat, thin squamous cells lining the mucosal surfaces of the head and neck. Depending on the site of origin, the disease exhibits varied symptoms, prognostic features, and treatment approaches.
Key Risk Factors for Head and Neck Squamous Cell Carcinoma
Several lifestyle and environmental exposures increase the risk of developing HNSCC:
- Tobacco Use: The leading cause of head and neck SCC.
- Alcohol Consumption: Acts synergistically with tobacco to increase risk.
- HPV Infection: Particularly HPV-16, associated with oropharyngeal cancers.
- Occupational Exposures: Wood dust, asbestos, and certain chemicals.
- Poor Oral Hygiene: Chronic inflammation may contribute to carcinogenesis.
- Dietary Deficiencies: Low intake of fruits and vegetables.
- Genetic Predisposition: Family history of head and neck cancers.
Common Symptoms of Squamous Cell Carcinoma of the Head and Neck
Symptoms vary by tumor location but typically include:
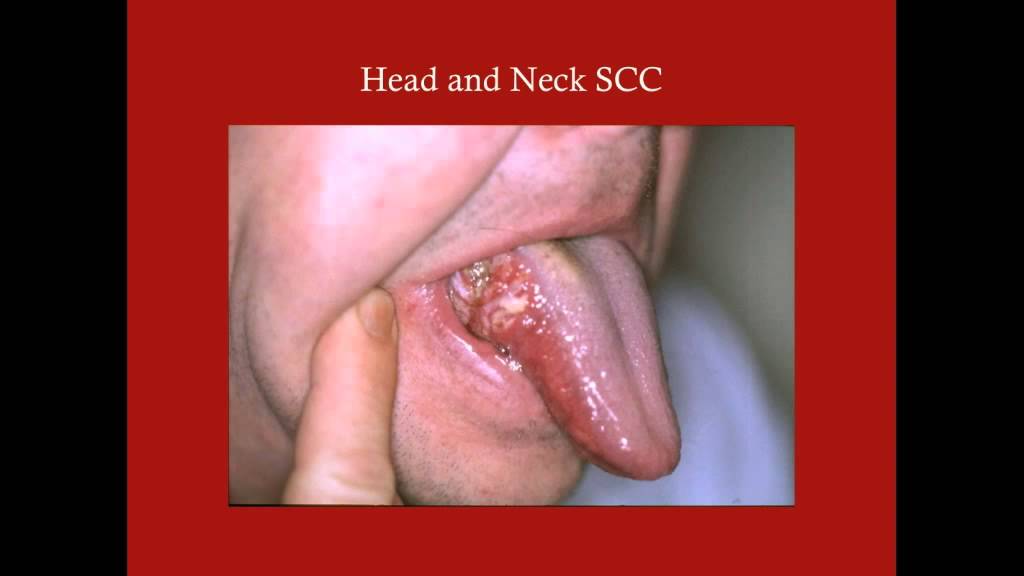
Oral Cavity
- Persistent mouth sore
- White or red patches (leukoplakia or erythroplakia)
- Jaw pain or loose teeth
Oropharynx
- Difficulty swallowing (dysphagia)
- Sore throat
- Lump in the neck
Larynx
- Hoarseness or voice changes
- Breathing difficulty
- Persistent cough
Nasopharynx and Hypopharynx
- Nasal obstruction
- Ear pain or hearing loss
- Epistaxis (nosebleeds)
Diagnostic Workup of Head and Neck Squamous Cell Carcinoma
Clinical Examination
- Comprehensive head and neck exam
- Palpation of cervical lymph nodes
Endoscopy
- Direct visualization and biopsy of suspicious mucosal lesions
Imaging Studies
- CT Scan: Assesses bone invasion and lymph node involvement
- MRI: Superior soft tissue detail
- PET-CT: Detects occult metastases and aids in staging
Biopsy and Pathology
- Confirmatory tissue diagnosis
- HPV testing for oropharyngeal tumors
- Immunohistochemistry for p16 expression
Staging of Squamous Cell Carcinoma: TNM Classification
Staging determines prognosis and guides treatment.
- T (Tumor): Size and extent of the primary lesion
- N (Node): Degree of regional lymph node involvement
- M (Metastasis): Presence of distant spread
AJCC TNM Staging Example:
| Stage | Description |
|---|---|
| I | Small, localized tumor |
| II | Larger tumor, no node involvement |
| III | Node-positive or extensive local growth |
| IV | Distant metastasis or advanced regional disease |
Treatment Modalities for Head and Neck Squamous Cell Carcinoma
The treatment strategy depends on tumor site, stage, HPV status, and patient factors.
Surgery
- Primary treatment for accessible and resectable tumors
- Neck dissection for lymph node involvement
- Reconstructive surgery may be necessary
Radiation Therapy
- Definitive or adjuvant treatment
- Intensity-modulated radiation therapy (IMRT) enhances precision
Chemotherapy
- Used in concurrent chemoradiotherapy (CCRT)
- Common agents: Cisplatin, 5-FU, Cetuximab
- Indicated for advanced or unresectable disease
Immunotherapy
- Checkpoint inhibitors (e.g., pembrolizumab, nivolumab) for recurrent/metastatic SCC
- Approved for PD-L1 positive tumors
Prognosis and Survival Outcomes
Prognosis varies significantly with stage and HPV status.
| Factor | Prognostic Implication |
|---|---|
| HPV-positive oropharyngeal SCC | Favorable response to treatment |
| Advanced T or N stage | Higher recurrence risk |
| Smoking history | Worse overall survival |
Five-year survival rates:
- Early-stage: >80%
- Advanced stage: 30–60%
- HPV-positive oropharyngeal: up to 90%
Preventive Strategies and Risk Reduction
- Smoking cessation and alcohol moderation
- HPV vaccination (recommended for ages 9–26)
- Oral health maintenance
- Regular screenings for high-risk individuals
- Occupational safety measures
Frequently Asked Questions:
Is squamous cell carcinoma of the head and neck curable?
Yes, especially when diagnosed at an early stage. Even advanced cases respond well to combined modality treatment.
How is HPV status relevant in SCC?
HPV-positive SCC, especially of the oropharynx, has better treatment response and prognosis than HPV-negative tumors.
Can SCC spread to other organs?
Yes, although distant metastasis is less common. The lungs, liver, and bones are potential sites of spread.
Is immunotherapy effective for head and neck SCC?
Yes. Immunotherapy is a standard option for recurrent/metastatic SCC, particularly with PD-L1 expression.
What is the role of diet in prevention?
A diet rich in antioxidants and fiber from fruits and vegetables may reduce the risk of developing head and neck cancers.
Squamous cell carcinoma of the head and neck remains a major global health challenge, with increasing incidence in HPV-associated cases. Early detection, multidisciplinary management, and evolving therapies such as immunotherapy offer hope for improved outcomes. Comprehensive awareness and preventive measures are crucial to reducing the burden of this potentially curable disease.