Rickettsialpox is an acute, self-limiting zoonotic disease caused by Rickettsia akari, a member of the spotted fever group (SFG) of Rickettsiae. It is transmitted to humans by the bite of infected mites—primarily the house mouse mite (Liponyssoides sanguineus). Despite its rarity, rickettsialpox remains a notable example of an urban rickettsial disease and is endemic in some metropolitan areas.

Causative Agent and Transmission Pathway
The Role of Rickettsia akari
R. akari is an obligate intracellular, Gram-negative bacterium that infects vascular endothelial cells. The organism is maintained in nature through a rodent-mite cycle, predominantly involving common house mice (Mus musculus) as reservoirs.
Vector: Liponyssoides sanguineus
This mite species feeds on infected mice and transmits the bacterium to humans through a painless bite, which often goes unnoticed until symptoms appear.
Epidemiology and Risk Factors
Though sporadic, rickettsialpox has been documented in major urban centers, including New York City, Eastern Europe, Korea, and parts of Russia. Outbreaks are often linked to rodent infestations in overcrowded residential areas or public buildings.
High-Risk Settings
- Poor sanitation or pest control
- Rodent-infested dwellings
- Dense urban populations
- Undiagnosed mite exposure
Clinical Manifestations of Rickettsialpox
Symptoms usually appear 7 to 10 days after the mite bite. The disease mimics varicella (chickenpox), leading to occasional misdiagnosis. Rickettsialpox progresses through distinct clinical phases:
Inoculation Site and Eschar Formation
- Begins as a small red papule
- Evolves into a blackened eschar (necrotic ulcer)
- Often accompanied by regional lymphadenopathy
Systemic Symptoms
| Symptom | Description |
|---|---|
| Fever | Abrupt onset, high-grade |
| Headache | Common and sometimes severe |
| Myalgia | General muscle aches |
| Chills and rigors | Accompanying the febrile episode |
| Malaise | Fatigue, lethargy |
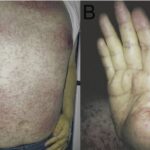
Vesicular Rash
- Appears 2–3 days after fever onset
- Resembles chickenpox with papulovesicular lesions
- Distributed on face, trunk, and extremities
- Resolves without scarring
Diagnostic Evaluation
Clinical Suspicion
Diagnosis is often clinical, particularly in endemic areas or among patients with a history of rodent exposure and eschar presence.
Laboratory Investigations
| Test | Utility |
|---|---|
| Indirect Immunofluorescence (IFA) | Most reliable serologic method for confirmation |
| PCR | Detects R. akari DNA in skin biopsy or blood |
| Skin Biopsy | Confirms rickettsial vasculitis via histopathology |
| Weil-Felix Test | Historically used, lacks specificity and sensitivity |
Differential Diagnosis
The symptoms of rickettsialpox can mimic several other diseases. It is crucial to differentiate it from:
- Varicella-zoster virus (chickenpox)
- Smallpox (in eradicated settings)
- Scrub typhus
- Anthrax (cutaneous)
- Other spotted fevers like Rocky Mountain spotted fever
Treatment and Prognosis
Antibiotic Therapy
- Doxycycline: 100 mg twice daily for 5–7 days (first-line treatment)
- Tetracycline: Alternative option, especially in older protocols
Treatment results in rapid symptom resolution, often within 48–72 hours.
Supportive Care
- Antipyretics for fever
- Adequate hydration
- Rest and monitoring for complications (rare)
Prognosis
- Excellent with appropriate antibiotic therapy
- No fatalities or severe complications in most documented cases
- Full recovery within 1–2 weeks
Prevention Strategies
Environmental Control
- Rodent extermination in infested buildings
- Regular inspection of residential and storage areas
- Proper garbage disposal to reduce rodent food sources
Personal Protective Measures
- Avoiding contact with rodents and infested materials
- Using insect repellents when in high-risk settings
- Prompt medical evaluation if symptoms appear after a suspected mite bite
Public Health Implications
Although rare, rickettsialpox represents an important urban health concern, especially in neglected communities. It emphasizes the intersection of infectious disease, pest control, and housing quality.
Key Points for Health Authorities
- Maintain rodent surveillance in urban housing units
- Educate healthcare providers in endemic regions
- Improve awareness and sanitation practices in at-risk populations
Rickettsialpox, caused by Rickettsia akari and transmitted through mite bites from infected rodents, is a mild yet clinically distinctive febrile illness. With early diagnosis and doxycycline therapy, outcomes are uniformly favorable. Public health initiatives focusing on vector control and urban hygiene are crucial in preventing future outbreaks.