Restless Leg Syndrome (RLS), also known as Willis-Ekbom Disease, is a neurological sensorimotor disorder characterized by an uncontrollable urge to move the legs. This urge typically intensifies during periods of rest or inactivity, particularly in the evening or at night, leading to sleep disturbances and significant reductions in quality of life.
Key Characteristics and Symptoms of RLS
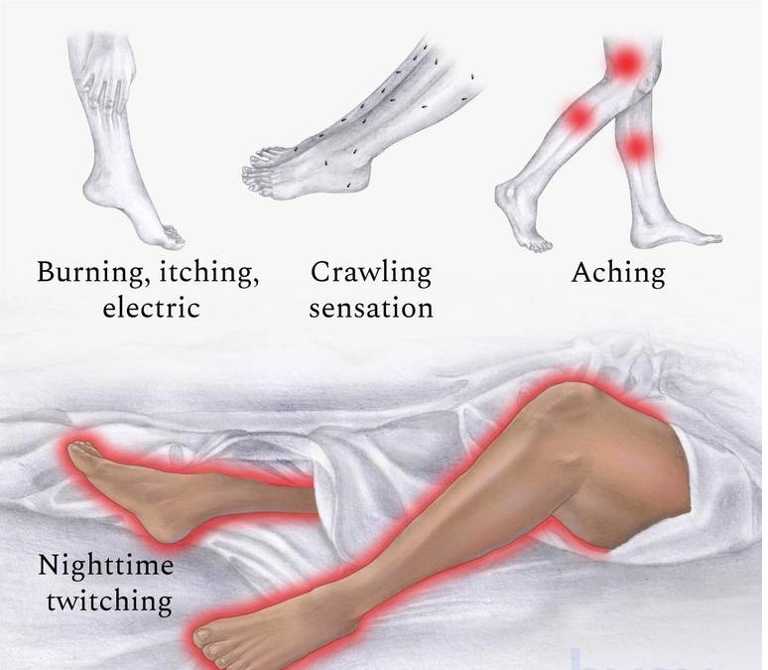
RLS is primarily defined by uncomfortable sensations in the legs, usually described as crawling, tingling, itching, pulling, or throbbing. The discomfort is typically alleviated by movement and worsens with prolonged sitting or lying down.
Core Symptoms Include:
- Strong urge to move the legs, often accompanied by unpleasant sensations
- Worsening of symptoms during rest or inactivity
- Relief through movement such as walking, stretching, or jiggling the legs
- Evening or nighttime predominance of symptoms
- Sleep disturbances, including difficulty falling or staying asleep
In severe cases, symptoms may affect the arms or occur during the daytime, significantly interfering with daily activities.
Underlying Causes and Risk Factors
RLS can be classified as primary (idiopathic) or secondary to other medical conditions. While the exact cause is not fully understood, it is believed to involve dysfunction in dopamine signaling and abnormalities in iron metabolism within the brain.
Primary RLS:
Often hereditary, with onset before age 40. Genetic predisposition plays a significant role, especially involving MEIS1, BTBD9, and MAP2K5 gene variants.
Secondary RLS:
Associated with underlying medical conditions or medications.
Common Risk Factors:
- Iron deficiency or low ferritin levels
- Chronic kidney disease
- Pregnancy (especially third trimester)
- Peripheral neuropathy
- Diabetes mellitus
- Rheumatoid arthritis
- Certain medications, including antihistamines, antidepressants, and antipsychotics
- Sleep deprivation and stress
Pathophysiology of RLS
The pathogenesis of RLS is believed to involve a disruption in dopaminergic pathways and brain iron homeostasis. Reduced dopamine activity in the basal ganglia and decreased iron levels in the substantia nigra contribute to the sensory and motor symptoms observed in RLS.
Diagnostic Criteria and Clinical Evaluation
Diagnosis of RLS is clinical and relies on patient history and symptom patterns. The International Restless Legs Syndrome Study Group (IRLSSG) outlines five essential diagnostic criteria:
- Urge to move the legs, often accompanied by unpleasant sensations
- Symptoms begin or worsen during rest or inactivity
- Partial or complete relief by movement
- Symptoms worsen in the evening or night
- Symptoms not solely accounted for by another condition (e.g., leg cramps, arthritis)
Additional Evaluation:
- Iron studies, including serum ferritin, transferrin saturation
- Renal function tests
- Polysomnography if sleep disorders are suspected
- Neurological examination to rule out neuropathies
Treatment Options for Restless Leg Syndrome
Treatment depends on the severity of symptoms and the presence of any underlying causes. The primary goals are to alleviate symptoms, improve sleep, and address contributing medical conditions.
1. Lifestyle and Behavioral Modifications
- Establishing a consistent sleep schedule
- Avoiding caffeine, nicotine, and alcohol
- Engaging in moderate, regular exercise
- Leg massages, warm baths, or heating pads
- Stress-reducing techniques such as yoga or meditation
2. Iron Supplementation
For patients with ferritin levels below 75 ng/mL, oral or intravenous iron therapy may be beneficial. Iron plays a key role in dopamine synthesis and brain function.
3. Pharmacological Treatments
Dopaminergic Agents:
- Pramipexole, Ropinirole, Rotigotine
- Effective in short-term relief but may lead to augmentation (worsening of symptoms over time)
Alpha-2-delta Calcium Channel Ligands:
- Gabapentin, Pregabalin
- Useful for painful RLS and comorbid insomnia
Opioids (for refractory cases):
- Oxycodone-naloxone, Tramadol
- Prescribed under strict supervision due to dependency risks
Benzodiazepines:
- Clonazepam, Temazepam
- Used primarily for sleep support
Management of RLS in Special Populations
Pregnancy:
RLS is common during pregnancy due to hormonal and iron changes. Treatment involves iron supplementation and conservative lifestyle adjustments. Pharmacological therapy is typically avoided unless symptoms are severe.
Children:
Diagnosis in children requires careful evaluation as symptoms may mimic growing pains or behavioral issues. Behavioral therapy and iron correction are primary strategies.
Elderly:
RLS may overlap with other age-related conditions. Careful medication management and non-pharmacologic therapies are prioritized.
Long-Term Outlook and Complications
If untreated, RLS can lead to chronic insomnia, depression, anxiety, and decreased quality of life. Augmentation, a paradoxical worsening of symptoms with continued use of dopamine agonists, is a major long-term complication that requires careful treatment adjustment.
Frequently Asked Questions:
1. Is restless leg syndrome a serious condition?
While not life-threatening, RLS can severely impact sleep and mental health, requiring proper management.
2. Can restless leg syndrome go away on its own?
Mild cases may improve with lifestyle changes, but persistent or worsening symptoms often require treatment.
3. What triggers restless leg syndrome?
Common triggers include iron deficiency, certain medications, pregnancy, prolonged inactivity, and lack of sleep.
4. Is there a cure for restless leg syndrome?
There is no definitive cure, but many effective treatments exist to manage and reduce symptoms.
5. Does exercise help with restless leg syndrome?
Yes, regular moderate physical activity is known to reduce symptom frequency and severity.