Mantle cell lymphoma (MCL) is a rare subtype of non-Hodgkin lymphoma (NHL) that originates from B lymphocytes within the mantle zone of lymphoid follicles. MCL is aggressive and often diagnosed at an advanced stage, making early recognition and intervention critical.
Causes and Risk Factors
MCL is primarily linked to genetic mutations, particularly the translocation t(11;14), which leads to overexpression of cyclin D1, promoting uncontrolled cell proliferation. Risk factors include:
- Age: More common in individuals over 60.
- Gender: Men are more frequently affected.
- Genetic predisposition: Family history of lymphomas.
- Environmental factors: Exposure to chemicals like pesticides may play a role.
Symptoms of Mantle Cell Lymphoma
MCL symptoms are often non-specific, leading to delayed diagnosis. Common symptoms include:
- Swollen lymph nodes (neck, armpits, or groin)
- Unexplained weight loss
- Fever and night sweats
- Loss of appetite
- Gastrointestinal involvement (diarrhea, bloating, or bleeding)
Diagnosis of MCL
Diagnosis requires a combination of clinical assessment, imaging, and laboratory tests:
1. Physical Examination and Medical History
A thorough physical exam identifies swollen lymph nodes and organ enlargement.
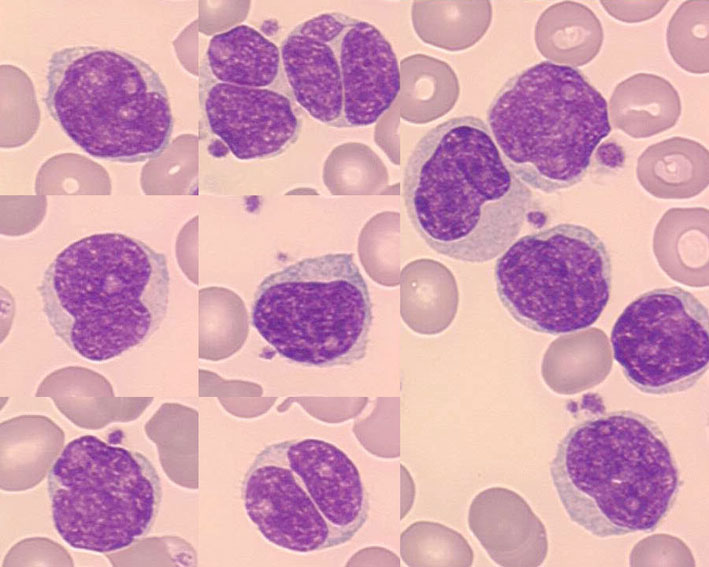
2. Biopsy and Histopathology
Lymph node or bone marrow biopsy confirms MCL. Immunohistochemistry detects cyclin D1 overexpression, a hallmark of MCL.
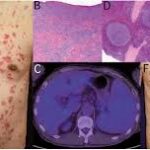
3. Imaging Studies
- CT Scan & PET Scan: Identify tumor spread.
- Endoscopy/Colonoscopy: Detect gastrointestinal involvement.
4. Genetic and Molecular Testing
Fluorescence in situ hybridization (FISH) and polymerase chain reaction (PCR) detect t(11;14) translocation.
Treatment Options
MCL treatment depends on disease stage and patient health. Common treatments include:
1. Chemotherapy
- R-CHOP regimen: Rituximab + cyclophosphamide, doxorubicin, vincristine, prednisone.
- Hyper-CVAD regimen: High-dose chemotherapy for aggressive cases.
2. Targeted Therapy
- Bruton’s tyrosine kinase (BTK) inhibitors: Ibrutinib, acalabrutinib.
- BCL-2 inhibitors: Venetoclax for relapsed MCL.
3. Immunotherapy
- Monoclonal antibodies (rituximab) enhance immune response against lymphoma cells.
4. Stem Cell Transplantation
- Autologous stem cell transplant (ASCT): Recommended for young patients with high-risk MCL.
5. Radiation Therapy
- Used for localized MCL or palliative care in advanced stages.
Prognosis and Survival Rates
MCL prognosis depends on age, stage, and response to therapy. The Mantle Cell Lymphoma International Prognostic Index (MIPI) helps predict survival:
- Low risk: Median survival >5 years.
- Intermediate risk: 3-5 years.
- High risk: <3 years.
Ongoing Research and Future Therapies
Emerging therapies include:
- Chimeric Antigen Receptor (CAR) T-cell Therapy
- Next-generation BTK inhibitors
- Personalized medicine and genomic-based treatments
Mantle cell lymphoma is an aggressive form of NHL requiring timely diagnosis and a multidisciplinary treatment approach. Advances in targeted therapy and immunotherapy offer new hope for improved outcomes.