Hereditary Factor XIII A subunit deficiency is a rare congenital bleeding disorder resulting from mutations in the F13A1 gene. This condition impairs the blood’s ability to form stable clots, leading to prolonged bleeding episodes and other complications.
What is Factor XIII A Subunit Deficiency?
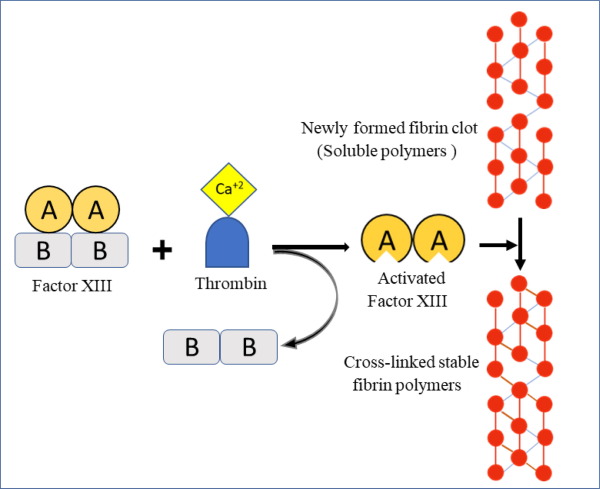
Factor XIII (FXIII) is a crucial clotting factor composed of two subunits: the A subunit (produced in the bone marrow) and the B subunit (produced in the liver). The A subunit plays a primary role in stabilizing blood clots by cross-linking fibrin molecules. A deficiency in this subunit results in poor clot formation and delayed wound healing.
Causes and Genetic Basis
Hereditary FXIII A subunit deficiency is an autosomal recessive disorder caused by mutations in the F13A1 gene. Both parents must carry a defective copy of the gene for their child to inherit the condition. Genetic mutations in the F13A1 gene reduce or completely eliminate the production of functional FXIII A subunits, impairing clot stability.
Symptoms of FXIII A Subunit Deficiency
Symptoms vary in severity and may include:
- Umbilical cord bleeding in newborns (a hallmark sign)
- Prolonged bleeding from minor injuries
- Spontaneous bruising
- Intracranial hemorrhage (potentially life-threatening)
- Poor wound healing
- Recurrent miscarriages in affected women
Diagnosis and Laboratory Testing
Early diagnosis is critical for managing FXIII A subunit deficiency. Common diagnostic methods include:
Clotting Time Tests
- Prothrombin Time (PT): Typically normal
- Activated Partial Thromboplastin Time (aPTT): Usually unaffected
Specific Factor XIII Assays
- Quantitative FXIII Assay: Determines FXIII activity levels
- Molecular Genetic Testing: Identifies mutations in the F13A1 gene
Treatment Options
Treatment focuses on restoring FXIII levels to prevent bleeding episodes.
FXIII Concentrate Replacement Therapy
- Plasma-derived FXIII Concentrate: The standard treatment option administered prophylactically or on-demand during bleeding episodes
- Recombinant FXIII (rFXIII): An effective alternative for patients requiring regular prophylaxis
Additional Management Strategies
- Fresh Frozen Plasma (FFP): Used in urgent bleeding scenarios
- Antifibrinolytic Agents: Supportive treatment to stabilize blood clots
- Wound Care: Specialized attention to minimize infection risk and promote healing
Potential Complications
If untreated, FXIII A subunit deficiency can lead to:
- Severe intracranial hemorrhage
- Recurrent pregnancy loss
- Persistent wound healing issues
Living with FXIII A Subunit Deficiency
Patients can lead relatively normal lives with appropriate management. Key recommendations include:
- Routine follow-ups with a hematologist
- Prophylactic treatments before surgeries or childbirth
- Wearing medical alert identification
FAQs
What is the primary cause of FXIII A subunit deficiency?
The condition is caused by mutations in the F13A1 gene, resulting in reduced or absent FXIII A subunit production.
How is FXIII A subunit deficiency diagnosed?
Diagnosis involves specific factor XIII assays, genetic testing, and clinical symptom evaluation.
Can FXIII A subunit deficiency be cured?
While there is no cure, effective management through FXIII concentrate replacement therapy ensures a stable quality of life.
Are children of carriers at risk of developing the condition?
Children inherit FXIII A subunit deficiency only if they receive defective genes from both parents.
What are the key symptoms of FXIII A subunit deficiency?
Common symptoms include umbilical cord bleeding in newborns, spontaneous bruising, and prolonged bleeding from minor cuts.
Hereditary FXIII A subunit deficiency is a manageable yet serious condition that requires timely diagnosis and ongoing treatment. Through appropriate therapy and proactive care, individuals with this rare disorder can minimize complications and maintain their quality of life.