Ductal carcinoma in situ (DCIS) is a non-invasive condition where abnormal cells are found in the milk ducts of the breast but have not spread beyond the duct walls. Although DCIS itself is not life-threatening, it can increase the risk of developing invasive breast cancer if left untreated. In this article, we will explore the causes, risk factors, symptoms, diagnosis, and treatment options for ductal carcinoma in situ, as well as its long-term prognosis.
Understanding Ductal Carcinoma in Situ (DCIS)
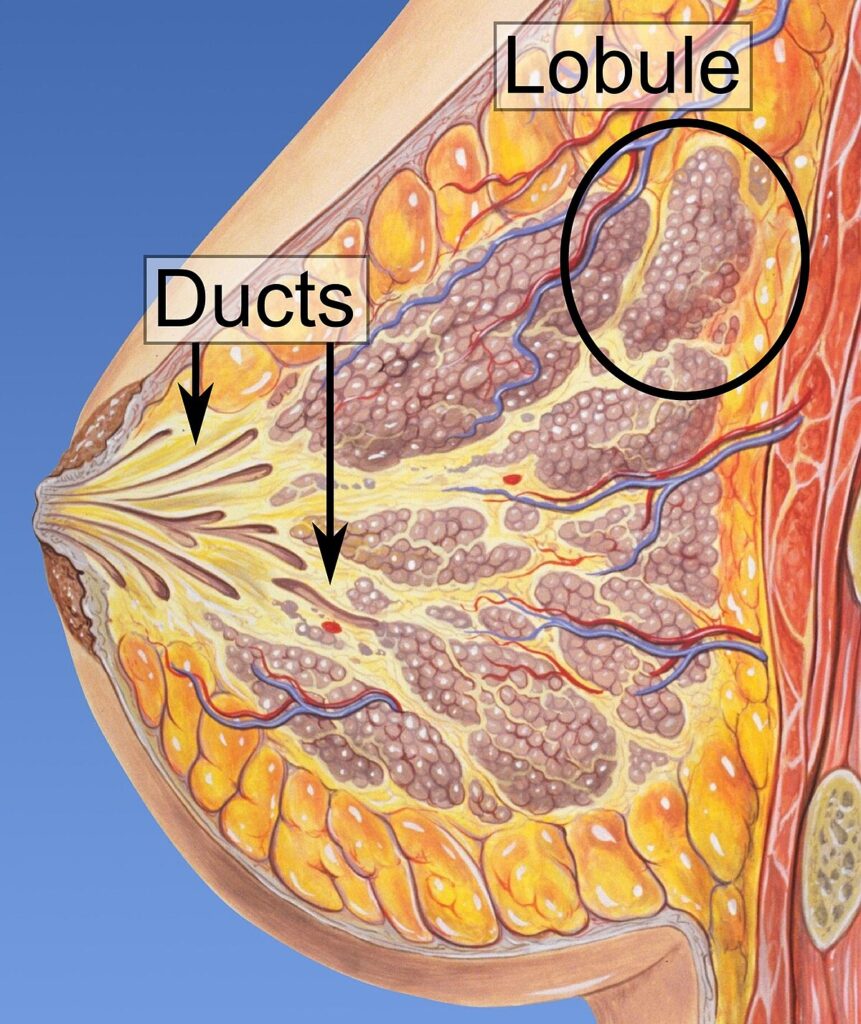
DCIS is often referred to as an early-stage or “pre-cancerous” form of breast cancer. It is characterized by the presence of abnormal cells that remain confined to the milk ducts of the breast and have not infiltrated surrounding tissues. Unlike invasive breast cancer, DCIS does not spread to other parts of the body, making it more treatable.
While DCIS is not considered an immediate threat to life, it requires medical intervention due to the potential for progression into invasive breast cancer over time. The risk of progression varies depending on the specific characteristics of the DCIS, including its grade and size.
Key Characteristics of DCIS
- Non-invasive: The abnormal cells are confined to the milk ducts.
- Asymptomatic in many cases: Most women with DCIS do not experience symptoms.
- Variable progression: Some cases of DCIS may never develop into invasive cancer, while others may progress more rapidly.
Risk Factors for Ductal Carcinoma in Situ
Several factors can increase the likelihood of developing ductal carcinoma in situ. These factors are not definitive causes but rather contributors that may elevate the risk. Some of the most common risk factors for DCIS include:
- Age: The risk of DCIS increases with age, particularly after menopause.
- Family History: A family history of breast cancer, especially in close relatives, may increase the likelihood of DCIS.
- Hormonal Factors: Hormone replacement therapy (HRT) and prolonged exposure to estrogen may increase the risk.
- Genetic Mutations: Mutations in genes such as BRCA1 and BRCA2 are strongly linked to a higher risk of breast cancer, including DCIS.
- Previous Radiation Exposure: Women who have undergone chest radiation therapy for conditions such as Hodgkin’s lymphoma may have an elevated risk of DCIS.
Symptoms of Ductal Carcinoma in Situ
Ductal carcinoma in situ is often asymptomatic, meaning that most women do not experience noticeable signs or symptoms. However, in some cases, DCIS may present with:
- Breast Lump: A palpable mass or thickening in the breast.
- Changes in the Skin: Alterations in the appearance of the skin, such as dimpling or puckering.
- Nipple Discharge: Unexplained discharge from the nipple, often clear or bloody.
- Pain or Tenderness: Although rare, some women may experience discomfort or pain in the affected breast.
Due to the asymptomatic nature of DCIS in most cases, routine screening through mammography is vital for early detection.
Diagnosis of Ductal Carcinoma in Situ
Early detection of DCIS plays a critical role in successful treatment. Diagnostic procedures for DCIS typically begin with imaging tests, followed by biopsy for confirmation. The following steps are commonly involved in the diagnosis of DCIS:
1. Mammography
Mammography is the most common and effective imaging technique used to detect abnormal growths in the breast. DCIS often appears as microcalcifications (tiny deposits of calcium) in the milk ducts. A mammogram can reveal these calcifications, but it cannot definitively determine whether they are cancerous.
2. Biopsy
Once a suspicious area is detected on a mammogram, a biopsy is performed to confirm the presence of DCIS. There are several types of biopsy techniques, including:
- Core Needle Biopsy: A needle is used to remove a small sample of tissue from the breast for examination.
- Stereotactic Biopsy: A type of biopsy that uses mammographic images to guide the needle to the abnormal tissue.
- Excisional Biopsy: A surgical procedure in which a portion of the breast tissue, including the suspected tumor, is removed for analysis.
3. Breast MRI
In some cases, a breast MRI may be used to obtain more detailed images of the breast tissue, especially if the DCIS is large or difficult to assess using mammography alone.
Treatment Options for Ductal Carcinoma in Situ
The treatment for ductal carcinoma in situ depends on various factors, including the size and location of the DCIS, the grade of the cells, and whether it is hormone receptor-positive. The main goal of treatment is to prevent the progression of DCIS to invasive breast cancer. The following are common treatment options for DCIS:
1. Surgical Treatment
Surgical intervention is the most common approach to treating DCIS. The two main types of surgery include:
- Breast-Conserving Surgery (Lumpectomy): The removal of the tumor and a small margin of surrounding healthy tissue. This is often followed by radiation therapy to reduce the risk of recurrence.
- Mastectomy: In cases where DCIS is widespread or recurring, a mastectomy may be recommended, which involves the removal of the entire breast.
2. Radiation Therapy
Radiation therapy is often recommended following breast-conserving surgery to kill any remaining cancer cells and reduce the risk of recurrence. This treatment may also be considered in cases where the DCIS is large or high-grade.
3. Hormone Therapy
If the DCIS is hormone receptor-positive, hormone therapy may be used to block the effects of estrogen and progesterone on cancer cells. Medications such as tamoxifen or aromatase inhibitors can be prescribed to lower the risk of recurrence, particularly in postmenopausal women.
4. Targeted Therapy
In some cases, targeted therapies that focus on specific characteristics of the tumor cells, such as HER2 status, may be recommended.
Prognosis and Long-Term Outlook for DCIS
The prognosis for ductal carcinoma in situ is generally favorable, particularly when the condition is detected early and treated appropriately. The survival rate for women with DCIS is very high, with most patients going on to live long, healthy lives after treatment. However, there is a small risk of recurrence, particularly in women with high-grade DCIS or those who do not undergo recommended treatments like radiation or hormone therapy.
Factors Affecting Prognosis
- Grade of DCIS: Higher-grade DCIS has a greater potential to progress into invasive cancer.
- Size of the Tumor: Larger DCIS tumors may have a higher risk of recurrence.
- Hormone Receptor Status: DCIS that is estrogen or progesterone receptor-positive typically responds well to hormone therapy, improving the prognosis.