Acute myeloid leukemia (AML) is an aggressive form of blood cancer characterized by the rapid proliferation of abnormal myeloid cells in the bone marrow and bloodstream. AML disrupts normal hematopoiesis, leading to anemia, infections, and bleeding disorders. The disease primarily affects older adults but can also occur in younger individuals and children.
Pathophysiology of Acute Myeloid Leukemia
AML arises due to genetic mutations in hematopoietic stem cells, leading to uncontrolled proliferation of immature white blood cells (blasts). These malignant cells accumulate in the bone marrow, suppressing the production of normal blood cells.
Risk Factors for Acute Myeloid Leukemia
Several factors increase the risk of developing AML, including:
- Age: Most common in individuals over 60.
- Genetic Disorders: Conditions like Down syndrome and Fanconi anemia.
- Radiation Exposure: Previous cancer treatments or high radiation exposure.
- Chemical Exposure: Benzene and other carcinogens.
- Previous Chemotherapy: Treatment for other cancers using alkylating agents or topoisomerase inhibitors.
- Myelodysplastic Syndromes (MDS): Pre-leukemic blood disorders.
Symptoms of Acute Myeloid Leukemia
- Fatigue and Weakness: Resulting from anemia.
- Frequent Infections: Due to a lack of functional white blood cells.
- Easy Bruising and Bleeding: Caused by thrombocytopenia (low platelet count).
- Unexplained Weight Loss: Common in malignancies.
- Bone Pain: Due to marrow expansion.
- Swollen Lymph Nodes and Enlarged Spleen/Liver: Occasional findings in AML.
Diagnosis of AML
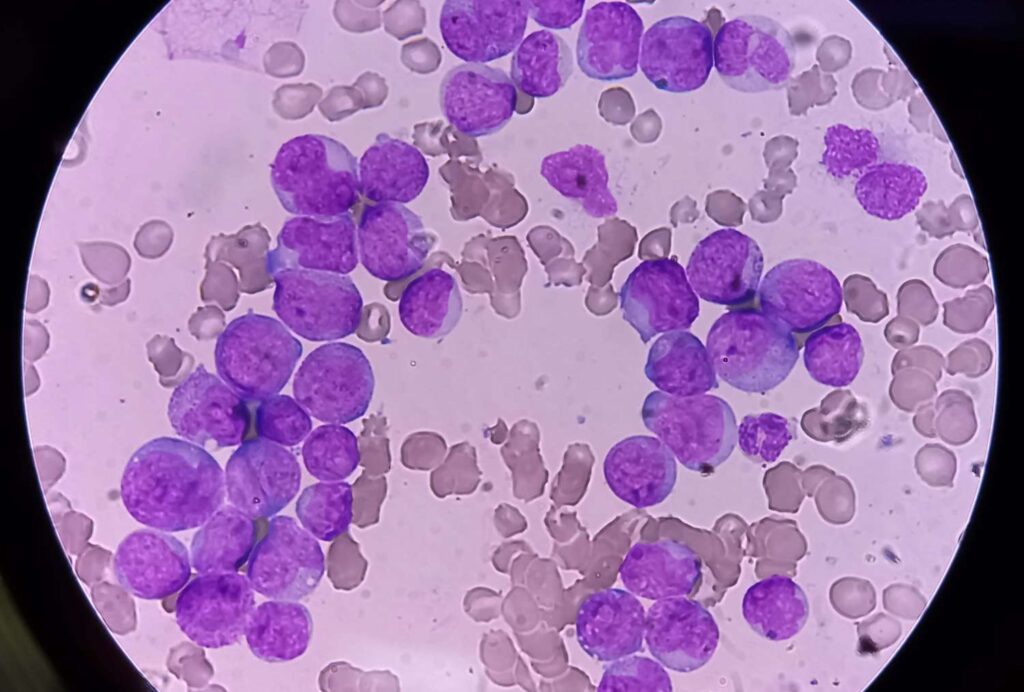
1. Complete Blood Count (CBC) and Peripheral Blood Smear
- High white blood cell count with circulating blast cells.
- Low red blood cell and platelet counts.
2. Bone Marrow Biopsy and Aspirate
- Confirms AML by revealing >20% blasts in the bone marrow.
3. Cytogenetic and Molecular Testing
- Identifies genetic mutations (e.g., FLT3, NPM1, CEBPA) to guide prognosis and treatment.
4. Flow Cytometry
- Determines cell surface markers to classify AML subtypes.
Treatment Strategies for Acute Myeloid Leukemia
1. Induction Chemotherapy
- Standard protocol: 7+3 regimen (7 days of cytarabine + 3 days of anthracycline).
- Goal: Achieve complete remission by eliminating leukemic cells.
2. Consolidation Therapy
- High-dose cytarabine (HiDAC) or allogeneic stem cell transplantation.
- Aims to eradicate residual disease and prevent relapse.
3. Targeted Therapy
- FLT3 inhibitors (e.g., midostaurin, gilteritinib) for FLT3-mutated AML.
- IDH inhibitors (enasidenib, ivosidenib) for IDH1/2 mutations.
- BCL-2 inhibitors (venetoclax) in combination with hypomethylating agents.
4. Stem Cell Transplantation
- Allogeneic Transplant: Preferred for high-risk AML patients.
- Autologous Transplant: Used in select cases of relapsed AML.
5. Supportive Care
- Transfusions: Red blood cells and platelets to manage anemia and bleeding.
- Growth Factors: G-CSF to stimulate white blood cell production.
- Infection Control: Antibiotics and antifungal prophylaxis.
Prognosis and Survival Rates
- Favorable Prognosis: Younger patients with core-binding factor mutations.
- Intermediate Prognosis: Normal cytogenetics with NPM1 or CEBPA mutations.
- Poor Prognosis: Complex karyotype, TP53 mutations, or secondary AML.
- 5-Year Survival Rate: 25-30% in older adults, 50-60% in younger patients.
Acute myeloid leukemia is an aggressive hematologic malignancy requiring prompt diagnosis and treatment. Advances in chemotherapy, targeted therapies, and stem cell transplantation have improved survival rates. Ongoing research into novel therapeutic approaches continues to provide hope for better patient outcomes.