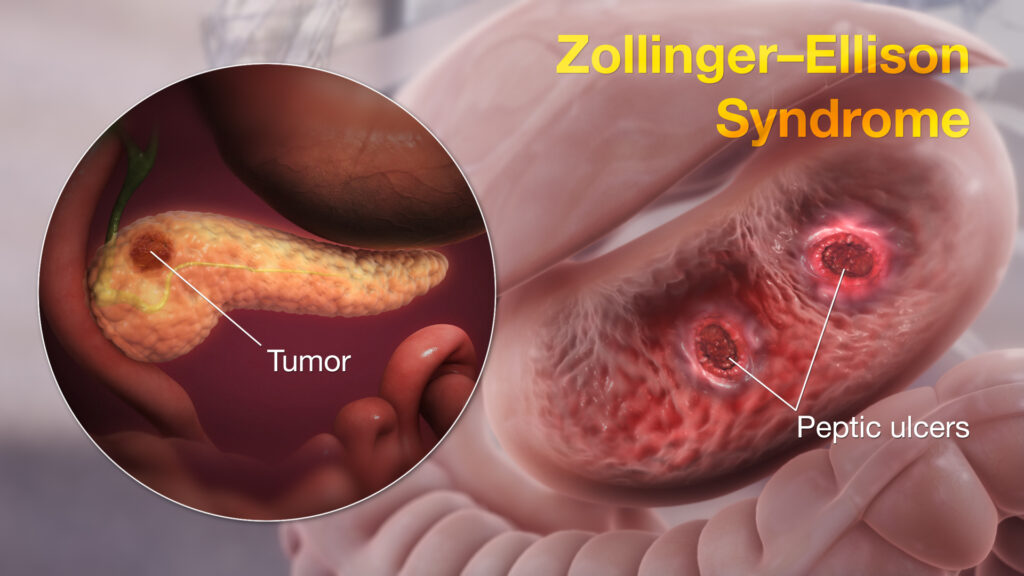
Zollinger-Ellison Syndrome (ZES) is a rare but serious disorder characterized by the formation of gastrin-secreting tumors, known as gastrinomas, primarily in the pancreas or duodenum. These tumors lead to excessive production of gastric acid, resulting in severe peptic ulcers, gastroesophageal reflux, and potential complications affecting the gastrointestinal tract. Early recognition and appropriate management are crucial to reduce morbidity and improve patient outcomes.
Understanding Zollinger-Ellison Syndrome
Zollinger-Ellison Syndrome involves the pathological overproduction of gastrin, a hormone that stimulates acid secretion in the stomach. The condition arises due to one or more gastrinomas—neuroendocrine tumors that can be malignant and metastasize, most commonly to the liver and lymph nodes.
Pathophysiology of Gastrinoma and Acid Hypersecretion
In individuals with ZES, gastrinomas lead to unregulated gastrin release, which significantly increases gastric acid secretion. The resultant hyperacidity damages the mucosal lining of the stomach and duodenum, causing ulcers and potentially leading to gastrointestinal bleeding or perforation.
Causes and Risk Factors
1. Sporadic Gastrinomas
Most cases of ZES are sporadic, occurring without a clear genetic predisposition.
2. Multiple Endocrine Neoplasia Type 1 (MEN1)
Approximately 25% of ZES cases are associated with MEN1, a hereditary condition that predisposes individuals to tumors of the endocrine glands, including the parathyroid, pituitary, and pancreas.
3. Genetic Factors
Inherited mutations, particularly in the MEN1 gene on chromosome 11, significantly increase the risk of gastrinoma development.
Clinical Symptoms of Zollinger-Ellison Syndrome
Symptoms often mimic those of common gastrointestinal disorders but are typically more severe and resistant to standard treatments.
- Recurrent peptic ulcers in the stomach and duodenum.
- Abdominal pain, especially postprandial.
- Chronic diarrhea due to acid-induced damage and malabsorption.
- Heartburn and acid reflux (GERD).
- Weight loss associated with malabsorption.
- Nausea and vomiting in advanced cases.
- Gastrointestinal bleeding, evident as hematemesis or melena.
Diagnostic Evaluation
1. Serum Gastrin Levels
Fasting serum gastrin levels exceeding 1,000 pg/mL are strongly suggestive of ZES, particularly when gastric pH is low (<2).
2. Secretin Stimulation Test
This confirmatory test distinguishes ZES from other causes of hypergastrinemia. In ZES, secretin paradoxically stimulates gastrin release.
3. Imaging Studies
- Somatostatin receptor scintigraphy (OctreoScan): Identifies gastrinomas by targeting somatostatin receptors.
- Endoscopic ultrasound (EUS): Detects small pancreatic and duodenal tumors.
- MRI or CT scans: Evaluate tumor size, location, and metastasis.
4. Gastric pH Measurement
Confirms acid hypersecretion, particularly when serum gastrin is modestly elevated.
Differentiating Zollinger-Ellison Syndrome from Other Disorders
ZES must be distinguished from other conditions with similar presentations, such as:
- Peptic ulcer disease (without hypergastrinemia).
- Helicobacter pylori infection.
- Chronic use of NSAIDs or corticosteroids.
- Atrophic gastritis or pernicious anemia (associated with high gastrin but low acid levels).
Management and Treatment Strategies
1. Proton Pump Inhibitors (PPIs)
High-dose PPIs such as omeprazole or pantoprazole are first-line to control gastric acid hypersecretion. Doses often exceed those used in standard GERD or ulcer therapy.
2. Surgical Resection of Gastrinoma
- Localized tumors may be surgically removed for potential cure.
- Duodenal exploration is essential due to the high likelihood of small, multiple tumors in that region.
- MEN1-associated ZES often involves multiple tumors, making complete resection challenging.
3. Medical Therapy for Metastatic Disease
- Somatostatin analogs (e.g., octreotide) to suppress gastrin secretion.
- Targeted therapies or chemotherapy for advanced or inoperable gastrinomas.
4. Management of MEN1
In patients with MEN1, a multidisciplinary approach is required to monitor and manage associated endocrine tumors.
Complications of Untreated Zollinger-Ellison Syndrome
- Perforated ulcers, which may require emergency surgical intervention.
- Gastrointestinal bleeding, potentially life-threatening.
- Strictures or obstruction due to chronic ulceration.
- Nutritional deficiencies due to malabsorption.
- Liver metastases, the most common site for spread of malignant gastrinomas.
Prognosis and Long-Term Outlook
The prognosis depends on:
- Presence of metastases at diagnosis.
- Response to medical therapy.
- Complete surgical resection of the tumor.
- MEN1 status: Prognosis may be more guarded due to the presence of multiple tumors and endocrine abnormalities.
With modern acid-suppressive therapy and timely surgical intervention, most patients achieve symptom control and improved quality of life.
Preventive Measures and Monitoring
- Genetic counseling and regular screening for MEN1 families.
- Lifelong monitoring with periodic imaging and serum gastrin levels.
- PPI therapy adjustments based on acid output and symptomatology.
- Nutritional assessments to detect deficiencies due to malabsorption.
