Tertiary yaws represents the chronic and disfiguring stage of yaws, a tropical infection caused by Treponema pallidum pertenue, a subspecies of the bacterium responsible for syphilis. Though early stages of yaws are marked by infectious skin lesions, the tertiary phase—typically occurring five or more years after initial infection—results in severe tissue destruction, primarily of the skin, cartilage, and bones. While largely eliminated in industrialized nations, tertiary yaws continues to affect remote, low-resource communities.
Overview of Yaws Progression and Tertiary Stage
The natural course of untreated yaws follows a progression through three clinical stages:
- Primary stage: Initial skin lesion or “mother yaw”
- Secondary stage: Multiple papillomatous lesions and lymphadenopathy
- Latent stage: Asymptomatic, yet serologically positive
- Tertiary stage: Non-infectious but debilitating gummatous and osteoarticular lesions
Etiology and Pathophysiology
Tertiary yaws is caused by the chronic persistence of T. pallidum pertenue in the host, resulting in a delayed hypersensitivity reaction rather than active infection. The bacteria stimulate a granulomatous immune response, leading to irreversible tissue damage, especially in bones and skin.
Clinical Manifestations of Tertiary Yaws
Tertiary yaws typically emerges 5 to 15 years after untreated primary or secondary stages. Unlike early yaws, the tertiary form is non-contagious, but it causes progressive and mutilating damage.
1. Gummatous Lesions
- Nodular or ulcerative lesions
- Affects skin and subcutaneous tissue
- Can become large, coalesce, and lead to scarring
- Common on the face, limbs, and back
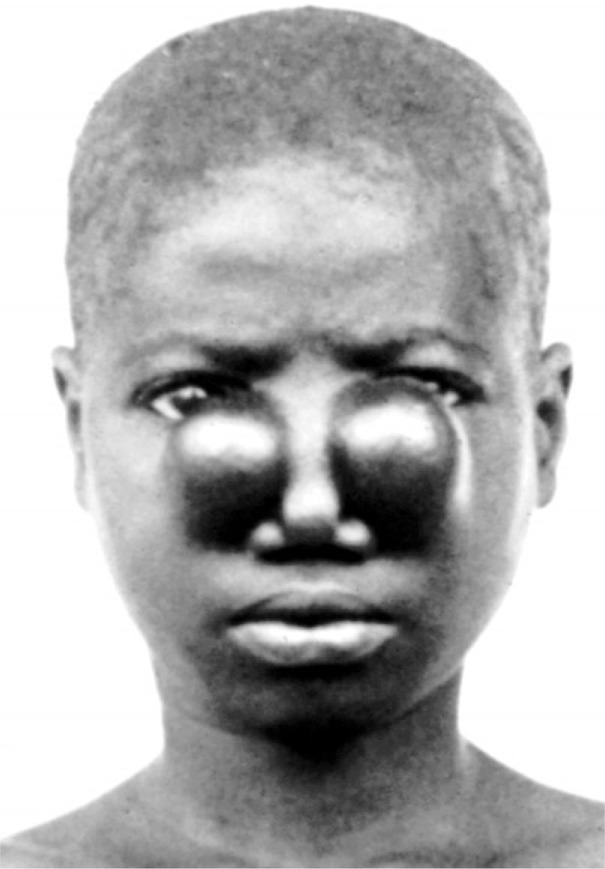
2. Gangosa (Mutilating Rhinopharyngitis)
- Involvement of nasal cartilage and bones
- Perforation of the nasal septum
- Collapse of the nasal bridge (saddle nose)
- Pharyngeal ulceration and facial deformity
3. Bone Involvement (Osteoperiostitis)
- Chronic periosteal thickening
- Bone swelling and bowing, particularly of the tibia and radius
- Painful deformities that can limit mobility
- Saber shins and frontal bossing in children
4. Disability and Social Stigma
- Disfigurement leads to functional limitations
- Long-term psychological and social impact
Diagnosis of Tertiary Yaws
Diagnosis requires clinical evaluation, serological confirmation, and exclusion of other causes of granulomatous or bone-destructive diseases.
Serological Testing
- Non-treponemal tests (e.g., VDRL, RPR): Quantify disease activity
- Treponemal tests (e.g., TPHA, FTA-ABS): Confirm infection; remain positive for life
Imaging Studies
- X-rays: Show bone thickening, periosteal reaction, and bowing
- MRI or CT scans: Used for complex anatomical involvement
Differential Diagnosis
| Condition | Similar Features | Differentiators |
|---|---|---|
| Leprosy | Skin lesions, deformity | Nerve thickening, acid-fast bacilli |
| Syphilis | Gummas, bone involvement | Genital lesions, sexual transmission |
| Tuberculosis | Granulomas, bone damage | Pulmonary symptoms, AFB in sputum |
| Fungal infections | Chronic skin lesions | Positive fungal cultures |
Treatment of Tertiary Yaws
Early treatment prevents progression; however, once tertiary yaws has developed, antibiotics halt the disease but do not reverse existing tissue damage.
First-Line Therapy
- Benzathine Penicillin G
- Adults: 1.2 million units IM weekly × 3 weeks
- Children: Adjusted by weight
Alternative Regimens (Penicillin Allergy)
- Azithromycin (30 mg/kg, max 2 g, single oral dose)
- Highly effective in early yaws, but efficacy in tertiary stage less documented
- Doxycycline or Erythromycin (14 days)
- Less preferred due to longer duration
Supportive Management
- Reconstructive surgery for nasal or facial deformities
- Physiotherapy for bone/joint involvement
- Community-based rehabilitation for social reintegration
Public Health Perspective
Epidemiology
- Yaws affects over 80 countries historically
- Most prevalent in tropical areas of Africa, Southeast Asia, and the Pacific
- Children under 15 are the most affected
Eradication Efforts
The WHO’s Morges Strategy targets yaws eradication using mass treatment campaigns with single-dose azithromycin.
Challenges
- Remote geographic areas with poor access to care
- Misdiagnosis with other granulomatous diseases
- Lack of consistent surveillance post-treatment
Complications of Untreated Tertiary Yaws
- Severe facial disfigurement
- Skeletal deformities
- Permanent disability
- Social exclusion
Without appropriate care, the disease contributes to lifelong morbidity and limits economic productivity, especially in endemic regions.
Prevention and Control
Primary Prevention
- Improve hygiene and living standards
- Health education campaigns
- Early identification and treatment of lesions
Secondary Prevention
- Mass Drug Administration (MDA) in endemic communities
- Contact tracing and treatment of family members
Tertiary Prevention
- Rehabilitative services
- Plastic and orthopedic surgery access
- Community support and psychological care
Frequently Asked Questions:
Is tertiary yaws contagious?
No. Unlike early-stage yaws, the tertiary stage is non-infectious and results from immune-mediated damage.
How long does it take for tertiary yaws to appear?
Typically 5 to 15 years after the initial infection if untreated.
Can tertiary yaws be reversed?
Antibiotics stop progression, but existing tissue damage is irreversible and requires supportive or surgical care.
What parts of the body are most affected?
Commonly affects the skin, nasal cartilage, pharynx, and long bones, leading to facial disfigurement and bone deformities.
How is tertiary yaws different from tertiary syphilis?
Tertiary yaws is non-venereal and predominantly affects the skin and bones, whereas tertiary syphilis may involve neurological or cardiovascular systems.
Tertiary yaws is a preventable but debilitating outcome of an untreated tropical infection. Through early intervention, effective antibiotic therapy, and public health surveillance, this disfiguring stage can be eliminated. Sustained global efforts, especially in endemic regions, remain essential to achieve the WHO’s goal of complete yaws eradication. Recognizing and addressing tertiary yaws not only alleviates individual suffering but also strengthens the fabric of underserved communities.

