The T3 suppression test is a specialized diagnostic tool employed in the evaluation of thyroid gland functionality, particularly in distinguishing between autonomous thyroid activity and normal regulatory function. This test assesses the pituitary-thyroid axis by observing the thyroid’s response to exogenous triiodothyronine (T3) administration.
Traditionally used in differentiating thyroid nodules or confirming subclinical hyperthyroidism, the T3 suppression test has largely been replaced in modern clinical practice by thyroid scintigraphy and TSH receptor antibody testing. However, in selected cases, particularly where imaging results are ambiguous, it retains diagnostic relevance.
Mechanism of T3 Suppression and Physiological Background
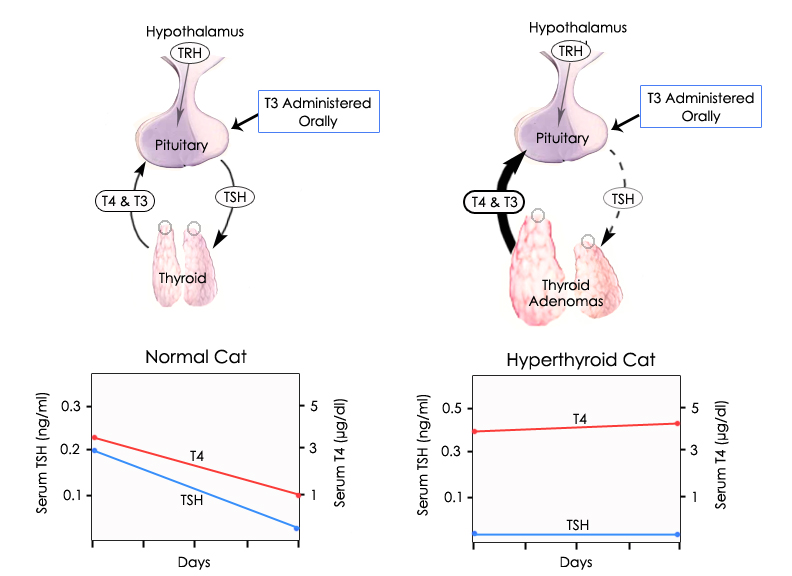
Under normal physiological conditions, elevated serum T3 levels exert negative feedback on the hypothalamic-pituitary-thyroid (HPT) axis, suppressing the secretion of thyroid-stimulating hormone (TSH) from the anterior pituitary. The T3 suppression test exploits this feedback loop to assess whether the thyroid gland’s activity is TSH-dependent.
In normal individuals:
- Administration of exogenous T3 leads to suppression of TSH.
- This results in reduced endogenous T4 and T3 production.
In patients with autonomous thyroid function (e.g., toxic nodules):
- The affected thyroid tissue continues to produce thyroid hormones independently of TSH regulation.
- No significant suppression of hormone production is observed despite elevated T3 levels.
Indications for the T3 Suppression Test
While not commonly used in routine practice today, the test has specific indications:
- Differentiation between benign euthyroid nodules and functioning thyroid adenomas
- Confirmation of autonomous thyroid function in borderline hyperthyroidism cases
- Assessment of pituitary TSH responsiveness in unusual or ambiguous thyroid profiles
Pre-Test Considerations and Patient Preparation
Prior to the T3 suppression test, a comprehensive baseline thyroid evaluation should be performed. This includes:
- TSH
- Free T3
- Free T4
- Thyroid ultrasound or radioiodine scan, if not previously done
Patient preparation:
- Discontinue any thyroid medications (levothyroxine, antithyroid drugs) at least 2 weeks prior, under physician guidance.
- Screen for cardiovascular risk; the test is contraindicated in patients with ischemic heart disease or arrhythmias.
- Obtain informed consent, especially due to the risk of inducing symptoms of hyperthyroidism.
T3 Suppression Test Protocol
Step-by-step procedure:
| Day | Procedure |
|---|---|
| 0 | Measure baseline serum TSH, T3, T4 |
| 1–7 | Administer liothyronine (T3) 25 mcg orally three times daily |
| 8 | Re-measure serum TSH, T3, T4 |
- Total daily dose of 75 mcg T3 is standard, continued for 7 days.
- Blood samples are collected before and after the suppression phase.
Interpretation of T3 Suppression Test Results
In Normal (TSH-Dependent) Thyroid Function:
- TSH: Suppressed to <0.1 mIU/L
- T4: Decreased or suppressed
- T3: Elevated due to exogenous intake
In Autonomous (TSH-Independent) Thyroid Function:
- TSH: Remains suppressed (baseline)
- T4: Remains elevated or unchanged
- T3: High due to external T3 but fails to suppress endogenous production
In Pituitary Abnormalities:
- No suppression of TSH, indicating non-functional pituitary feedback
Clinical Utility in Detecting Autonomous Nodules
Autonomous functioning thyroid nodules (AFTNs), often presenting as “hot nodules” on scintigraphy, continue to produce thyroid hormones regardless of TSH. The T3 suppression test confirms the autonomy by showing failure to suppress despite high circulating T3 levels.
This can aid in differentiating:
- Autonomous adenoma from multinodular goiter
- True hyperthyroidism from laboratory artifact or subclinical dysfunction
Risks and Contraindications
Although generally safe in healthy individuals, the T3 suppression test carries risks in patients with underlying comorbidities.
Contraindications:
- Cardiovascular disease (angina, arrhythmia, heart failure)
- Elderly patients with frailty
- Pregnancy or breastfeeding
- Known hyperthyroidism
Adverse effects:
- Palpitations, tremors
- Anxiety, insomnia
- Headaches or heat intolerance
Alternatives to the T3 Suppression Test
Modern thyroid diagnostics often replace the T3 suppression test with less invasive and more reliable modalities:
- Thyroid scintigraphy (radioiodine scan)
- TSH receptor antibody assays
- Ultrasound with Doppler flow studies
- Serum thyroglobulin measurement (for nodule surveillance)
These alternatives provide quicker, safer insights into thyroid autonomy and glandular activity.
The T3 suppression test remains a valuable investigative tool in select thyroid disorders, especially when imaging studies are inconclusive or in resource-limited settings. By evaluating TSH suppression in response to T3, it provides insights into the integrity of the hypothalamic-pituitary-thyroid axis and the autonomy of thyroid tissue.
However, due to its invasive nature, potential risks, and the availability of modern alternatives, its use should be reserved for carefully selected cases under expert supervision.

