Streptococcus acute otitis media (AOM) is a common bacterial infection of the middle ear, primarily caused by Streptococcus pneumoniae, a leading pathogen in pediatric ear infections. Characterized by rapid onset of ear pain, fever, and tympanic membrane inflammation, this condition predominantly affects children under five years of age but can occur in all age groups.
Pathophysiology: How Streptococcus Causes Ear Infections
Streptococcus pneumoniae, a Gram-positive diplococcus, colonizes the nasopharynx and ascends the Eustachian tube, especially during upper respiratory infections. Once in the middle ear, it multiplies, inducing inflammation and fluid accumulation, leading to the classic symptoms of acute otitis media.
Epidemiology and Risk Factors
Age and Seasonality
- Most prevalent in children aged 6 months to 3 years
- Peak incidence during autumn and winter
Key Risk Factors:
- Attendance in daycare
- Lack of breastfeeding
- Exposure to tobacco smoke
- Craniofacial anomalies (e.g., cleft palate)
- Family history of recurrent otitis media
S. pneumoniae is implicated in 25–50% of bacterial AOM cases, followed by Haemophilus influenzae and Moraxella catarrhalis.
Clinical Presentation of Streptococcus AOM
Cardinal Symptoms:
- Otalgia (ear pain)—often sudden and severe
- Fever ≥ 38°C
- Irritability and crying in infants
- Hearing loss or fullness in the ear
- Otorrhea (if tympanic membrane ruptures)
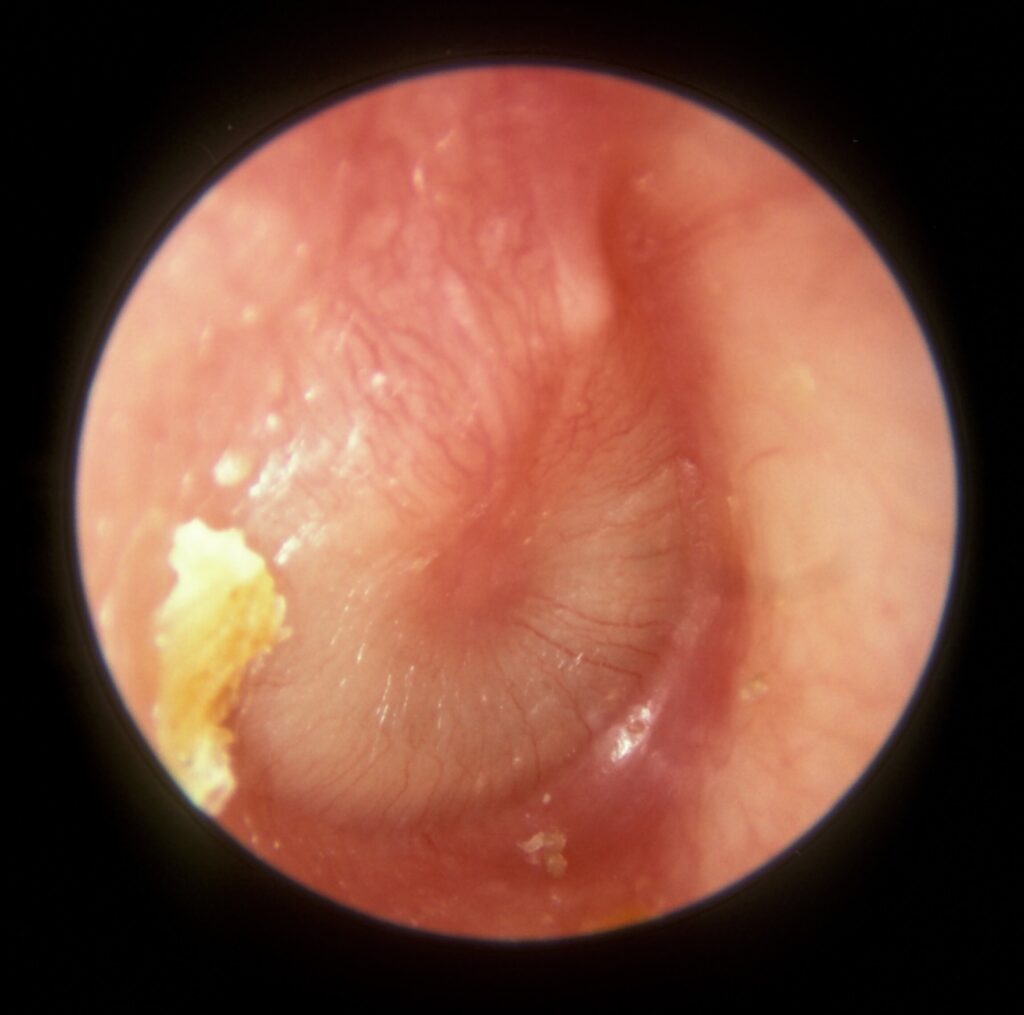
Physical Examination Findings:
- Bulging, erythematous tympanic membrane
- Decreased mobility on pneumatic otoscopy
- Possible presence of purulent middle ear effusion
Diagnosis is primarily clinical, based on the presence of middle ear effusion and signs of acute inflammation.
Diagnostic Approach
Clinical Diagnosis:
The American Academy of Pediatrics recommends diagnosis based on the following:
- Moderate to severe bulging of the tympanic membrane OR
- New-onset otorrhea not due to otitis externa OR
- Mild bulging with recent ear pain (within 48 hours) or intense erythema
Microbiological Testing:
- Tympanocentesis: Gold standard for pathogen isolation, reserved for refractory or complicated cases
- Nasopharyngeal cultures: Less reliable, used in research or epidemiologic surveillance
Antibiotic Treatment of Streptococcal AOM
First-Line Therapy:
- Amoxicillin: 80–90 mg/kg/day divided BID
Effective against penicillin-sensitive strains of S. pneumoniae
Alternative Agents:
- Amoxicillin-clavulanate: If beta-lactamase–producing organisms suspected
- Cefdinir, Cefuroxime, Cefpodoxime: For penicillin-allergic patients (non-anaphylactic)
- Clindamycin or macrolides: For true penicillin allergy
Duration of Therapy:
- 10 days: For children <2 years or with severe symptoms
- 7 days: For mild/moderate symptoms in 2–5 years
- 5–7 days: For children ≥6 years with mild symptoms
Watchful Waiting vs Immediate Antibiotic Use
In selected patients with mild disease, a watchful waiting approach (48–72 hours) is endorsed to reduce unnecessary antibiotic use.
Criteria for Watchful Waiting:
- Children ≥6 months
- Non-severe symptoms (mild otalgia <48 hours, temperature <39°C)
- Reliable follow-up access
This approach is not recommended for children <6 months or with bilateral AOM and otorrhea.
Recurrent and Chronic Otitis Media
Recurrent AOM:
- ≥3 episodes in 6 months or ≥4 episodes in 12 months with at least 1 in the past 6 months
Management Options:
- Tympanostomy tube placement
- Long-term low-dose prophylactic antibiotics (rarely recommended)
- Pneumococcal and influenza vaccination
Chronic middle ear effusion without infection may require audiological evaluation and possible surgical intervention.
Complications Associated with Streptococcus AOM
Though most cases resolve without issue, S. pneumoniae is associated with more severe and invasive complications, such as:
- Mastoiditis
- Tympanic membrane perforation
- Hearing loss
- Meningitis (via contiguous spread)
- Facial nerve paralysis
Prompt recognition and treatment mitigate the risk of long-term sequelae.
Preventive Strategies
Immunization:
- Pneumococcal conjugate vaccine (PCV13 or PCV15): Reduces nasopharyngeal colonization by S. pneumoniae
- Influenza vaccine: Lowers incidence of secondary bacterial otitis media
Environmental Modifications:
- Avoid exposure to secondhand smoke
- Encourage exclusive breastfeeding for at least 6 months
- Limit daycare attendance when feasible
Streptococcus acute otitis media remains a major cause of morbidity among children, driven by Streptococcus pneumoniae’s ability to colonize and invade the middle ear during viral infections. Optimal management requires accurate clinical assessment, judicious antibiotic use, and preventive vaccination. Recognizing high-risk cases, adhering to evidence-based treatment protocols, and pursuing surgical options when appropriate are essential to prevent recurrence and complications.

