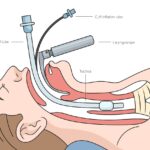
In cesarean section (C-section) procedures, rapid and effective airway management is critical. Endotracheal intubation, facilitated by skeletal muscle relaxants, ensures adequate oxygenation and ventilation while minimizing aspiration risk. The selection of a neuromuscular blocking agent must balance rapid onset, short duration, and minimal fetal transfer.
Importance of Rapid Sequence Induction in Cesarean Delivery
Rapid sequence induction (RSI) is the standard approach to general anesthesia for C-sections. Pregnant patients are considered to have a full stomach due to delayed gastric emptying, increasing the risk of pulmonary aspiration. RSI involves the administration of an induction agent followed immediately by a fast-acting muscle relaxant to enable swift intubation.
Key Objectives of RSI in Obstetrics:
- Prevent maternal hypoxia
- Minimize time to secure airway
- Reduce risk of aspiration
- Preserve uteroplacental perfusion
Pharmacological Agents for Skeletal Muscle Relaxation
Suxamethonium (Succinylcholine)
Suxamethonium remains the gold standard for skeletal muscle relaxation during RSI in obstetric patients.
Pharmacodynamics:
- Onset: 30–60 seconds
- Duration: 4–6 minutes
- Metabolism: Rapid hydrolysis by plasma cholinesterase
- Advantages: Quick onset and short duration permit rapid intubation with spontaneous recovery if needed
Considerations:
- Contraindicated in patients with pseudocholinesterase deficiency or risk of hyperkalemia
- May cause transient fetal bradycardia due to maternal fasciculations
Rocuronium
Rocuronium is a non-depolarizing alternative to suxamethonium, suitable for RSI when reversal agents like sugammadex are available.
Pharmacodynamics:
- Onset: 60–90 seconds (at higher doses, ~1.2 mg/kg)
- Duration: 30–60 minutes
- Reversal: Rapid with sugammadex (within 2–3 minutes)
Advantages:
- No fasciculations or rise in intraocular/intragastric pressures
- Lower incidence of bradycardia compared to suxamethonium
Considerations:
- Requires appropriate dosing to achieve comparable onset
- Reversal agent (sugammadex) must be readily available for emergent return of spontaneous ventilation
Comparative Overview
| Parameter | Suxamethonium | Rocuronium (1.2 mg/kg) |
|---|---|---|
| Type | Depolarizing | Non-depolarizing |
| Onset | 30–60 seconds | 60–90 seconds |
| Duration | 4–6 minutes | 30–60 minutes |
| Reversibility | Spontaneous | Sugammadex required |
| Fetal transfer | Minimal | Minimal |
| Adverse effects | Bradycardia, fasciculations, hyperkalemia | None significant in healthy individuals |
Factors Influencing Muscle Relaxant Choice in C-Section
Maternal Physiology
Pregnancy-induced physiological changes impact drug distribution and metabolism:
- Increased cardiac output and plasma volume
- Reduced plasma protein concentration
- Altered hepatic and renal clearance
These changes may accelerate onset but prolong recovery, necessitating precision in drug dosing.
Fetal Safety
All medications administered to the mother can cross the placenta to varying degrees. Agents like suxamethonium, due to their rapid metabolism and quaternary structure, have minimal fetal effects. Rocuronium’s molecular weight and low lipid solubility also limit placental transfer.
Urgency of Delivery
In emergency cesarean sections, time to secure the airway is critical. Suxamethonium is typically favored in these scenarios. In planned or elective procedures with adequate preparation, rocuronium may be used safely, especially when paired with sugammadex.
Monitoring Neuromuscular Blockade in Obstetric Patients
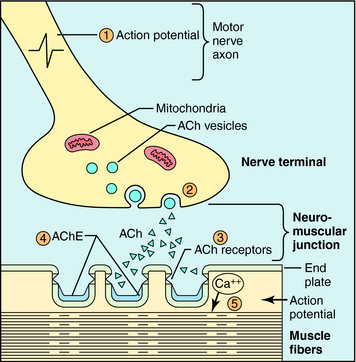
Neuromuscular transmission monitoring, such as train-of-four (TOF) stimulation, should be employed to assess the depth and recovery of muscle relaxation. Intraoperative monitoring ensures adequate intubation conditions and avoids prolonged paralysis postoperatively.
Best Practices and Recommendations
- Preferred agent for RSI in emergency C-section: Suxamethonium (unless contraindicated)
- Alternative agent when suxamethonium is contraindicated: Rocuronium with sugammadex availability
- Always monitor neuromuscular blockade intraoperatively
- Ensure multidisciplinary preparedness for neonatal resuscitation
Effective skeletal muscle relaxation for endotracheal intubation in cesarean sections is paramount for maternal and fetal safety. Suxamethonium remains the first-line agent due to its rapid onset and short duration, especially in emergent scenarios. Rocuronium is a viable alternative when paired with sugammadex, offering a non-depolarizing option with favorable safety and efficacy. The choice must be individualized, guided by clinical context, patient-specific factors, and drug availability.