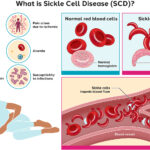
Sickle cell disease (SCD) with crisis represents the acute, life-threatening episodes that occur in individuals with SCD, often requiring urgent medical intervention. These crises are primarily caused by vascular occlusion due to abnormally shaped red blood cells obstructing blood flow. The two most severe forms are vaso-occlusive crisis (VOC) and acute chest syndrome (ACS), though other types of crises also pose serious health risks.
Pathophysiology: The Mechanism Behind Sickle Cell Crisis
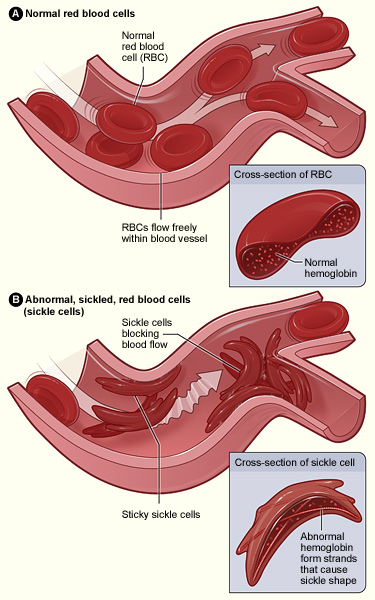
SCD is caused by a point mutation in the HBB gene, which produces hemoglobin S. Under hypoxic conditions, hemoglobin S polymerizes, distorting red blood cells into a sickle shape. These sickled cells lose flexibility, adhere to the endothelium, and cause microvascular blockages that result in ischemia and pain.
Types of Sickle Cell Crises
1. Vaso-Occlusive Crisis (VOC)
This is the most common type of sickle cell crisis, characterized by severe pain in the back, chest, abdomen, or extremities.
Key Features:
- Triggered by dehydration, infection, stress, cold weather
- Pain may last hours to days
- Often requires opioid analgesics and hydration
2. Acute Chest Syndrome (ACS)
ACS is a medical emergency resulting from sickling in the pulmonary vasculature.
Symptoms:
- Chest pain
- Fever
- Cough
- Hypoxia
- Lung infiltrates on imaging
3. Splenic Sequestration Crisis
Sudden pooling of blood in the spleen, mainly in children.
Clinical Indicators:
- Rapidly enlarging spleen
- Hypotension
- Severe anemia
4. Aplastic Crisis
Triggered by parvovirus B19 infection, leading to temporary suppression of red cell production.
Hallmarks:
- Profound anemia
- Reticulocytopenia
- Fatigue and pallor
5. Hemolytic Crisis
Excessive destruction of sickled RBCs leading to jaundice and worsening anemia.
Recognizing Symptoms of Sickle Cell Crisis
- Sudden, intense pain unrelieved by over-the-counter medications
- Fever, cough, or chest discomfort (suggestive of ACS)
- Shortness of breath or difficulty breathing
- Abdominal distension (possible splenic sequestration)
- Unusual fatigue, pale skin, or dizziness
- Signs of stroke (e.g., facial drooping, slurred speech)
Diagnosis and Evaluation
Laboratory Investigations:
- CBC: Reveals anemia, leukocytosis during crisis
- Reticulocyte count: Elevated in hemolytic and VOC, low in aplastic crisis
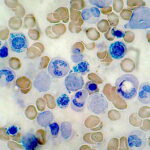
- Blood smear: Shows sickled cells
- LDH and bilirubin: Elevated due to hemolysis
- Arterial blood gases (ABG): Assess oxygenation in ACS
Imaging:
- Chest X-ray: To detect infiltrates in ACS
- Ultrasound: Evaluate spleen size in sequestration
- MRI/CT scan: Rule out stroke or avascular necrosis
Emergency Management of Sickle Cell Crisis
1. Pain Management
- Immediate administration of opioids (e.g., morphine, hydromorphone)
- Adjunctive use of NSAIDs when appropriate
- Use of PCA (patient-controlled analgesia) in hospitalized patients
2. Hydration Therapy
- IV fluids to reduce blood viscosity
- Oral hydration encouraged when stable
3. Oxygen Therapy
- Administered to manage hypoxia and prevent HbS polymerization
4. Antibiotics
- For suspected or confirmed infections, particularly in ACS
5. Blood Transfusions
- Simple or exchange transfusions in severe anemia, ACS, or stroke
- Monitor for iron overload in repeated transfusions
Long-Term Management to Prevent Crises
Pharmacologic Interventions:
- Hydroxyurea: Increases fetal hemoglobin (HbF) and reduces VOC frequency
- L-glutamine: Decreases oxidative stress and crisis incidence
- Voxelotor and Crizanlizumab: Target hemoglobin polymerization and adhesion respectively
Preventive Care:
- Routine vaccinations (influenza, pneumococcus, meningococcus)
- Penicillin prophylaxis in children under five
- Annual transcranial Doppler (TCD) ultrasound in children to prevent stroke
Lifestyle Modifications:
- Maintain hydration and a balanced diet
- Avoid cold exposure and high altitudes
- Regular exercise within tolerance
- Prompt management of infections
Complications Arising from Recurrent Crises
- Chronic pain and opioid dependency
- Pulmonary hypertension
- Renal failure
- Osteonecrosis of joints
- Retinopathy and vision loss
- Leg ulcers and delayed wound healing
- Cognitive impairment from silent cerebral infarcts
Gene Therapy and Curative Options
Hematopoietic Stem Cell Transplant (HSCT):
- Curative potential in pediatric patients with matched sibling donors
- Risk of graft-versus-host disease and transplant rejection
Emerging Gene Therapy:
- CRISPR-Cas9 editing of BCL11A or HBB gene
- Lentiviral gene addition approaches
- Clinical trials show promise for long-term remission
Sickle Cell Disease with Crisis: Global Health Perspective
SCD disproportionately affects populations in sub-Saharan Africa, India, the Middle East, and African Americans in the United States. Despite medical advances, mortality remains high in low-resource settings due to poor access to diagnostics and acute care.
Strategic Interventions:
- Implementation of universal newborn screening
- Education programs for early symptom recognition
- Expansion of access to hydroxyurea and transfusion services
- Development of SCD registries for better health planning
Prognosis and Quality of Life
With consistent and proactive management, many individuals with SCD can lead productive lives. The introduction of disease-modifying therapies and curative procedures has significantly improved survival rates. Multidisciplinary care teams involving hematologists, pain specialists, and psychologists are essential for optimal outcomes.
Sickle cell disease with crisis represents a significant clinical burden requiring timely recognition and aggressive intervention. Early diagnosis, comprehensive care, and access to emerging therapies are vital in reducing morbidity and improving the lives of those affected by this complex condition.