Sedation in intubated patients is a cornerstone of intensive care, ensuring patient comfort, synchrony with mechanical ventilation, and minimizing agitation-induced complications. An individualized, protocol-driven approach to sedation optimizes outcomes, shortens ICU stays, and improves mortality when combined with effective pain control and delirium prevention.

Goals of Sedation in the Intubated Patient
- Alleviate anxiety and distress
- Ensure ventilator synchrony
- Facilitate nursing care and procedures
- Prevent accidental extubation or catheter removal
- Promote sleep and reduce oxygen consumption
- Enable neuroprotection in select neurologic injuries
Sedation Depth: Tailoring to Clinical Needs
Sedation levels must be matched to the patient’s condition and ICU goals. Light sedation is now preferred in most non-neurologic cases due to its association with reduced complications.
| Sedation Depth | Description | Application |
|---|---|---|
| Minimal | Patient responsive to verbal commands | Weaning, cooperative ventilated states |
| Moderate | Purposeful response to tactile stimulation | Initial mechanical ventilation |
| Deep | Unresponsive except to painful stimuli | ARDS, high ICP, status epilepticus |
| Comatose (RASS -5) | No response to voice or pain | Neuromuscular blockade, severe agitation |
Preferred Target: RASS -2 to 0 in most ICU ventilated patients, unless contraindicated.
Common Sedative Agents Used in Intubated Patients
Propofol
- Advantages: Rapid onset/offset, easy titration, anticonvulsant
- Risks: Hypotension, hypertriglyceridemia, Propofol Infusion Syndrome (PRIS)
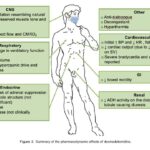
Dexmedetomidine
- Advantages: Minimal respiratory depression, anxiolytic, facilitates communication
- Ideal For: Light sedation and delirium prevention
Benzodiazepines (Midazolam, Lorazepam)
- Advantages: Anxiolysis, anticonvulsant
- Risks: Delirium, accumulation, prolonged sedation
Ketamine
- Advantages: Preserves airway reflexes, bronchodilation, analgesia
- Ideal For: Hemodynamically unstable patients, refractory status asthmaticus
Opioids (Fentanyl, Morphine)
- Role: Analgesia with secondary sedative effect
- Caution: Respiratory depression, ileus
Sedation Protocols and Daily Interruption
Benefits of Protocol-Driven Sedation:
- Shorter time on mechanical ventilation
- Reduced ICU length of stay
- Lower incidence of delirium
Daily Sedation Interruption (DSI) is recommended unless contraindicated, allowing for neurological assessments and promoting early mobilization.
ABCDEF Bundle Integration:
- A: Assess pain
- B: Both spontaneous awakening and breathing trials
- C: Choice of analgesia and sedation
- D: Delirium monitoring
- E: Early mobility
- F: Family engagement
Monitoring Sedation in Intubated Patients
Effective sedation monitoring ensures optimal depth while avoiding oversedation or awareness.
Sedation Scales:
- RASS (Richmond Agitation-Sedation Scale): Standard for ICU
- SAS (Sedation Agitation Scale): Alternative scale
- BIS (Bispectral Index): EEG-based tool for deeper sedation levels
Physiologic Monitoring:
- Heart rate variability, respiratory rate, blood pressure
- End-tidal CO₂ and oxygen saturation
- Neurologic assessment during sedation breaks
Managing Sedation-Related Complications
| Complication | Cause | Prevention/Management |
|---|---|---|
| Delirium | Benzodiazepines, deep sedation | Light sedation, dexmedetomidine, sleep hygiene |
| Prolonged Ventilation | Over-sedation | Daily sedation interruption, reassessment |
| Hypotension | Propofol or high-dose sedatives | Fluid resuscitation, dose adjustment |
| Withdrawal | Abrupt cessation of long use | Gradual weaning, symptom control |
| Respiratory Depression | Opioids, benzodiazepines | Avoid polypharmacy, monitor closely |
Special Considerations in Sedation Strategy
Neurologic Injury
- Deep sedation may be required for ICP control
- BIS and pupillary monitoring assist in titration
ARDS Patients
- Deeper sedation may improve ventilator compliance
- Often combined with neuromuscular blockade
COVID-19 and Prolonged Ventilation
- Prolonged deep sedation often necessary
- Emphasis on minimizing cumulative benzodiazepine exposure
Tapering and Weaning Off Sedation
Gradual reduction in sedation should parallel improvements in patient status:
- Decrease infusion rates incrementally
- Perform regular RASS assessments
- Initiate spontaneous breathing trials
- Consider transitioning to enteral agents (e.g., lorazepam)
Avoid abrupt cessation in prolonged sedation to prevent withdrawal syndromes.
Sedation in intubated patients is an intricate balance of pharmacologic expertise, continuous assessment, and individualized care. Adherence to evidence-based protocols, use of lighter sedation when appropriate, and multidisciplinary coordination are essential to improving patient outcomes in the intensive care setting. Through diligent monitoring and strategic pharmacologic choices, we ensure optimal comfort, safety, and recovery for mechanically ventilated individuals.