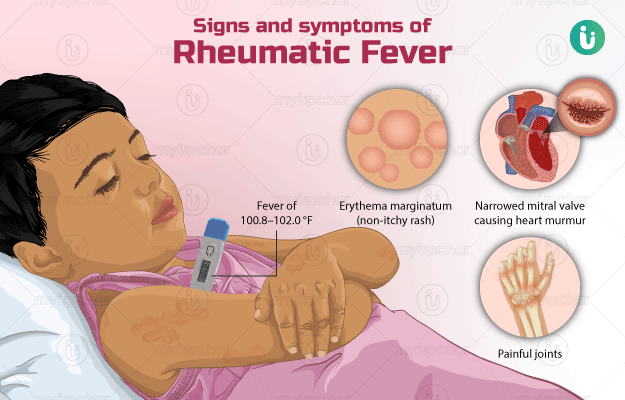
Rheumatic fever (RF) is a serious inflammatory condition that arises as a delayed autoimmune response to untreated or inadequately treated Group A streptococcal (GAS) pharyngitis. Despite being entirely preventable, it remains a global health burden, particularly in low-resource settings. Preventive measures, when implemented systematically, are highly effective in reducing the incidence of rheumatic fever and its most devastating sequela, rheumatic heart disease (RHD).
The Importance of Prevention: Avoiding Chronic Cardiac Complications
Prevention of rheumatic fever not only reduces morbidity and mortality but also significantly lessens healthcare costs associated with long-term management of cardiac damage. As rheumatic fever is a disease that develops following a known bacterial trigger, prevention is achievable at both the primary and secondary levels.
Primary Prevention: Treating Streptococcal Pharyngitis Promptly
Identification and Treatment of Group A Strep Infections
The cornerstone of primary prevention is the accurate and timely diagnosis of GAS pharyngitis followed by appropriate antibiotic therapy. This intervention halts the autoimmune cascade before it begins.
- Symptoms of Strep Throat:
- Sudden sore throat without cough
- Fever
- Swollen cervical lymph nodes
- Tonsillar exudates
- Diagnostic Tools:
- Rapid antigen detection tests (RADTs)
- Throat culture (gold standard)
- Recommended Treatment:
- Penicillin V: 250 mg orally 2–3 times daily for 10 days
- Amoxicillin: 50 mg/kg once daily (max 1 g/day) for 10 days
- For penicillin-allergic patients: Azithromycin or cephalexin
Proper adherence to a full 10-day antibiotic course is crucial to prevent immune-mediated complications.
Secondary Prevention: Long-Term Prophylaxis After First Rheumatic Fever Episode
Purpose of Secondary Prophylaxis
Patients with a confirmed diagnosis of rheumatic fever are at high risk for recurrence, especially in the first 5 years. Secondary prophylaxis aims to prevent recurrent GAS infections and further cardiac damage.
Recommended Regimens for Secondary Prophylaxis
- Intramuscular Benzathine Penicillin G: 1.2 million units every 3–4 weeks
- Oral Penicillin V: 250 mg twice daily (for those who refuse injections)
- Alternatives for Allergy: Erythromycin 250 mg twice daily
Duration of Prophylaxis
| Patient Condition | Duration of Prophylaxis |
|---|---|
| RF without carditis | 5 years or until age 21 (whichever is longer) |
| RF with carditis, no residual heart disease | 10 years or until age 21 (whichever is longer) |
| RF with carditis and persistent valvular disease | At least 10 years or until age 40; possibly lifelong |
Tertiary Prevention: Managing and Monitoring Established RHD
Though not true “prevention,” tertiary strategies are critical to preventing complications in those with established RHD.
- Regular echocardiographic surveillance
- Endocarditis prophylaxis before dental/surgical procedures
- Timely surgical valve repair or replacement
Public Health Measures: Community and System-Level Interventions
In endemic areas, prevention of rheumatic fever extends beyond clinical care to include public health infrastructure.
School and Community Programs
- Mass sore throat screening campaigns
- Educational initiatives about the importance of treating sore throats
- Training of primary healthcare workers in GAS diagnosis and treatment
National RF Prevention Programs
Countries like Cuba and Costa Rica have demonstrated dramatic declines in RF incidence through structured national strategies involving:
- Surveillance
- Free antibiotic availability
- Public health awareness campaigns
Barriers to Effective Rheumatic Fever Prevention
Despite the efficacy of known interventions, several barriers hinder implementation:
- Lack of awareness among patients and healthcare providers
- Antibiotic non-adherence
- Limited access to diagnostics in rural regions
- Supply chain issues for intramuscular penicillin
Overcoming these barriers requires coordinated action between health ministries, international health organizations, and community leaders.
Preventing rheumatic fever is an achievable goal with profound implications for global health. Through primary prevention via prompt antibiotic treatment, secondary prevention through sustained prophylaxis, and comprehensive public health policies, we can dramatically reduce the incidence of this debilitating disease. An integrated approach, combining individual treatment with systemic public health strategies, holds the key to eliminating rheumatic fever as a public health threat.

