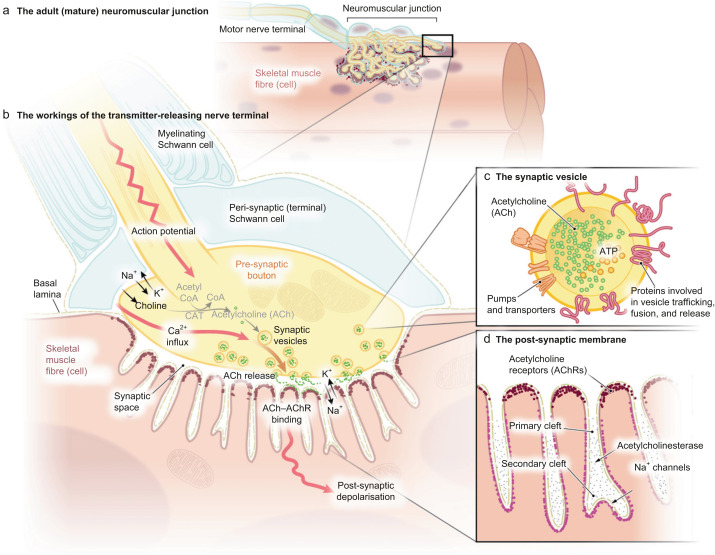
Nondepolarizing neuromuscular blocking agents (NMBAs) are widely used during general anesthesia to facilitate intubation and provide optimal surgical conditions. Common agents in this class include rocuronium, vecuronium, atracurium, and cisatracurium. These drugs function as competitive antagonists of acetylcholine at nicotinic receptors in the neuromuscular junction.
While essential in anesthesia, residual neuromuscular blockade (RNMB) after surgery can result in serious complications such as hypoventilation, airway obstruction, aspiration, and postoperative pulmonary issues. Hence, timely and appropriate reversal of nondepolarizing neuromuscular blockade is critical to ensure patient safety and optimal recovery.
Mechanism of Action: Nondepolarizing Neuromuscular Blocking Drugs
Nondepolarizing agents bind to acetylcholine receptors without activating them, preventing depolarization and muscle contraction. Unlike depolarizing agents like succinylcholine, these drugs do not cause fasciculations and have longer durations of action, necessitating pharmacologic reversal.
Reversal Strategies: Pharmacological Options and Monitoring
Key Agents for Reversal
1. Neostigmine
A traditional acetylcholinesterase inhibitor that increases acetylcholine concentration, competing with the NMBA at the neuromuscular junction.
- Indications: Moderate recovery (TOF count ≥2).
- Dosing: 0.04–0.07 mg/kg IV.
- Co-administration: Must be given with anticholinergic agents (e.g., glycopyrrolate 0.01 mg/kg) to counteract muscarinic side effects such as bradycardia and secretions.
- Limitations: Ineffective in deep blockade; risk of paradoxical weakness if used improperly.
2. Sugammadex
A selective relaxant binding agent (SRBA) designed specifically to reverse aminosteroidal NMBAs like rocuronium and vecuronium.
- Mechanism: Encapsulates NMBA molecules, rendering them inactive and facilitating renal excretion.
- Dosing:
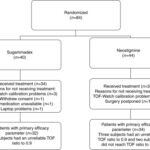
- TOF 2/4: 2 mg/kg
- Post-tetanic count 1–2: 4 mg/kg
- Immediate reversal (3 min post-intubation): 16 mg/kg
- Benefits: Rapid, predictable reversal even from profound blockade. No need for anticholinergics.
Neuromuscular Monitoring: Guiding Reversal Decisions
Train-of-Four (TOF) Stimulation
Objective neuromuscular monitoring is essential to assess the depth of blockade and determine the appropriate reversal strategy.
| TOF Count | Clinical Interpretation |
|---|---|
| 0/4 | Deep blockade |
| 1–2/4 | Moderate blockade |
| 4/4 with fade | Incomplete recovery |
| TOF Ratio ≥ 0.9 | Adequate recovery for extubation |
Best Practice:
We strongly recommend using quantitative neuromuscular monitoring (acceleromyography) rather than visual or tactile assessments alone.
Clinical Considerations and Special Populations
Renal Impairment
- Sugammadex: Prolonged elimination in severe renal dysfunction; use caution or avoid.
- Neostigmine: Safely used; requires careful monitoring for bradycardia and bronchial secretions.
Hepatic Dysfunction
- Vecuronium/Rocuronium: May have prolonged action; monitor closely.
- Reversal agents: No specific dose adjustments, but delayed onset possible with hepatic clearance impairments.
Pediatric and Geriatric Use
- Sugammadex: Approved for children ≥2 years old; dosing is weight-based.
- Neostigmine: Effective in all age groups; anticholinergic co-administration is mandatory.
Adverse Effects and Contraindications
Sugammadex
- Hypersensitivity reactions (rare but documented)
- Bradycardia (may require atropine)
- Caution in severe renal failure (CrCl < 30 mL/min)
Neostigmine
- Bradycardia, increased secretions, nausea, vomiting
- Cholinergic crisis with excessive dosing
- Requires adjunct anticholinergic
Optimizing Reversal Outcomes
Key Recommendations
- Avoid routine dosing without TOF confirmation
- Refrain from administering neostigmine during deep blockade (TOF <2)
- Ensure TOF ratio ≥ 0.9 prior to extubation
- Implement institutional guidelines for reversal timing, monitoring, and documentation
- Educate anesthesia teams on agent-specific use and monitoring protocols
Frequently Asked Questions:
Can neostigmine reverse deep neuromuscular blockade?
No. It is only effective when partial recovery has occurred (TOF ≥2/4).
Is sugammadex effective for all nondepolarizing agents?
No. It only reverses aminosteroidal agents like rocuronium and vecuronium.
What is the safest TOF ratio for extubation?
A TOF ratio ≥ 0.9 ensures sufficient neuromuscular recovery for safe extubation.
Do all patients need reversal agents?
Yes, unless full spontaneous recovery is confirmed objectively.
Can sugammadex be given without TOF monitoring?
It should not be. While effective, dosing accuracy depends on blockade depth.
Reversal of neuromuscular blockade induced by nondepolarizing agents demands a systematic, evidence-based approach. With advancements in pharmacology and monitoring, sugammadex has transformed clinical practice by providing fast and complete reversal of aminosteroidal NMBAs. Meanwhile, neostigmine remains a useful tool in selected cases with partial recovery. Objective monitoring with TOF and adherence to standardized reversal protocols ensure safe emergence from anesthesia and reduce postoperative complications.