Neuromuscular blocking agents (NMBAs) are essential in modern anesthesia, facilitating endotracheal intubation and optimal surgical conditions by inducing skeletal muscle paralysis. These agents are classified into depolarizing (e.g., succinylcholine) and non-depolarizing agents (e.g., rocuronium, vecuronium, cisatracurium).
Timely and effective reversal of neuromuscular blockade is critical to prevent residual neuromuscular blockade (RNMB), a condition associated with impaired respiratory function, hypoxia, aspiration, and postoperative complications.
Indications for NMBA Reversal
We advocate for reversal of neuromuscular blockade in the following contexts:
- Restoration of spontaneous breathing at the end of surgery
- Prevention of residual paralysis and airway complications
- Patient readiness for extubation
- Enhanced recovery protocols
- Unanticipated short surgical durations requiring rapid reversal
Primary Reversal Agents: Sugammadex vs. Neostigmine
Sugammadex: Selective Relaxant Binding Agent
Sugammadex is a modified γ-cyclodextrin specifically designed to encapsulate and inactivate aminosteroidal NMBAs like rocuronium and vecuronium.
Mechanism of Action:
Sugammadex forms a tight 1:1 complex with rocuronium or vecuronium, rendering the drug inactive and allowing rapid return of neuromuscular function.
Dosing Protocol:
| Depth of Blockade | TOF Count | Sugammadex Dose |
|---|---|---|
| Moderate (reappearance of T2) | 2/4 | 2 mg/kg |
| Deep (post-tetanic count 1–2) | 0/4 | 4 mg/kg |
| Immediate reversal (3 min post-rocuronium) | N/A | 16 mg/kg |
Advantages:
- Rapid, predictable reversal
- Effective in deep blockade
- No cholinergic side effects
- Well-tolerated profile
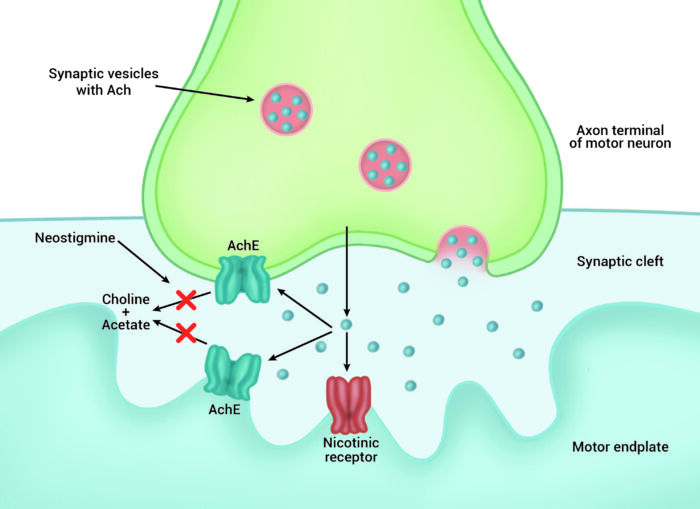
Neostigmine: Acetylcholinesterase Inhibitor
Neostigmine reverses non-depolarizing neuromuscular blockade by inhibiting acetylcholinesterase, increasing acetylcholine concentration at the neuromuscular junction.
Key Considerations:
- Only effective when some spontaneous recovery has occurred (TOF ≥ 2/4)
- Requires co-administration with anticholinergic agents (e.g., glycopyrrolate or atropine) to mitigate bradycardia, secretions, and GI side effects
Dosing Protocol:
| Clinical Recovery Level | Neostigmine Dose | Anticholinergic |
|---|---|---|
| TOF ≥ 2 | 0.04–0.07 mg/kg IV | Glycopyrrolate 0.01 mg/kg |
Limitations:
- Slower onset compared to sugammadex
- Ceiling effect limits efficacy in deep blockade
- Risk of paradoxical muscle weakness if administered too early
Objective Neuromuscular Monitoring: The TOF Ratio
Train-of-four (TOF) stimulation is the standard method to evaluate neuromuscular recovery.
| TOF Count | Clinical Correlation |
|---|---|
| 0/4 | Profound blockade |
| 1–2/4 | Deep blockade |
| 3/4 | Moderate blockade |
| 4/4 with fade | Incomplete recovery |
| TOF ratio ≥ 0.9 | Full recovery, safe for extubation |
Reversal in Special Clinical Situations
Pediatric Population
- Sugammadex is approved for children ≥2 years
- Dose adjustments based on weight
- Neostigmine remains an alternative with close monitoring
Geriatric Patients
- Pharmacodynamics of both agents largely preserved
- Slower renal clearance of sugammadex may prolong half-life
Renal Impairment
- Sugammadex: Use with caution in severe renal dysfunction; prolonged excretion and drug recirculation
- Neostigmine: No adjustment needed but monitor for bradycardia and secretions
Adverse Effects and Safety Considerations
Sugammadex:
- Rare cases of bradycardia, hypersensitivity, and anaphylaxis
- Avoid in patients with severe renal failure (CrCl < 30 mL/min)
Neostigmine:
- Cholinergic side effects: bradycardia, bronchospasm, nausea
- Requires co-administration with antimuscarinics
Clinical Implications and Best Practices
- Always use quantitative neuromuscular monitoring to guide reversal
- Avoid empiric dosing without TOF data
- Ensure TOF ratio ≥ 0.9 before extubation to prevent residual paralysis
- Implement reversal protocols in all surgical departments to standardize care
- Educate staff on drug-specific indications, dosing, and monitoring
Frequently Asked Questions:
Can sugammadex be used for cisatracurium-induced blockade?
No. Sugammadex is not effective for benzylisoquinolinium NMBAs like cisatracurium.
How soon after rocuronium can sugammadex be given?
Immediate reversal is possible with 16 mg/kg dosing within 3 minutes post-induction.
Is TOF monitoring mandatory before reversal?
Yes. TOF ratio ensures proper timing and dosing of reversal agents.
Can neostigmine be used in deep blockade?
No. Neostigmine is ineffective when TOF count is less than 2/4.
What if reversal is incomplete after sugammadex?
Repeat dosing may be necessary in very rare cases; ensure renal function is adequate.
Effective reversal of neuromuscular blockade is a cornerstone of modern anesthesia safety. The advent of sugammadex has significantly advanced our capacity to rapidly and reliably reverse aminosteroidal NMBAs, even from profound blockade. Meanwhile, neostigmine remains a viable option when used judiciously and in conjunction with anticholinergics. Adherence to evidence-based protocols, neuromuscular monitoring, and patient-specific considerations are essential to prevent complications and enhance postoperative recovery.