Recurrent aphthous stomatitis (RAS) is a common oral mucosal disorder characterized by recurring, painful ulcers, typically on non-keratinized oral tissues. Though benign and non-contagious, RAS can significantly impair quality of life by affecting eating, speaking, and oral hygiene. It is essential to understand its multifactorial etiology for effective management.
Etiology and Risk Factors for Recurrent Aphthous Stomatitis
The precise cause of RAS remains unclear; however, several contributing factors have been identified:
- Genetic Predisposition: Family history significantly increases susceptibility.
- Immune Dysregulation: Aberrant immune responses against oral mucosal antigens.
- Nutritional Deficiencies: Deficiencies in iron, folic acid, vitamin B12, and zinc.
- Local Trauma: Biting the cheek, orthodontic braces, or dental procedures.
- Hormonal Influences: Fluctuations during menstrual cycles.
- Stress and Anxiety: Psychological factors have been strongly correlated.
- Allergies: Hypersensitivity reactions to foods such as chocolate, coffee, or gluten.
- Underlying Systemic Diseases: Behçet’s disease, celiac disease, inflammatory bowel disease, and HIV infection.
Types of Recurrent Aphthous Stomatitis
RAS is classified into three clinical types based on ulcer characteristics:
- Minor Aphthous Ulcers:
- Diameter less than 10 mm
- Heal within 7–14 days without scarring
- Major Aphthous Ulcers:
- Diameter greater than 10 mm
- Deeper lesions, healing over several weeks with potential scarring
- Herpetiform Ulcers:
- Multiple small ulcers (1–3 mm) clustering together
- Resemble herpes simplex infections but are unrelated
Clinical Manifestations of Recurrent Aphthous Stomatitis
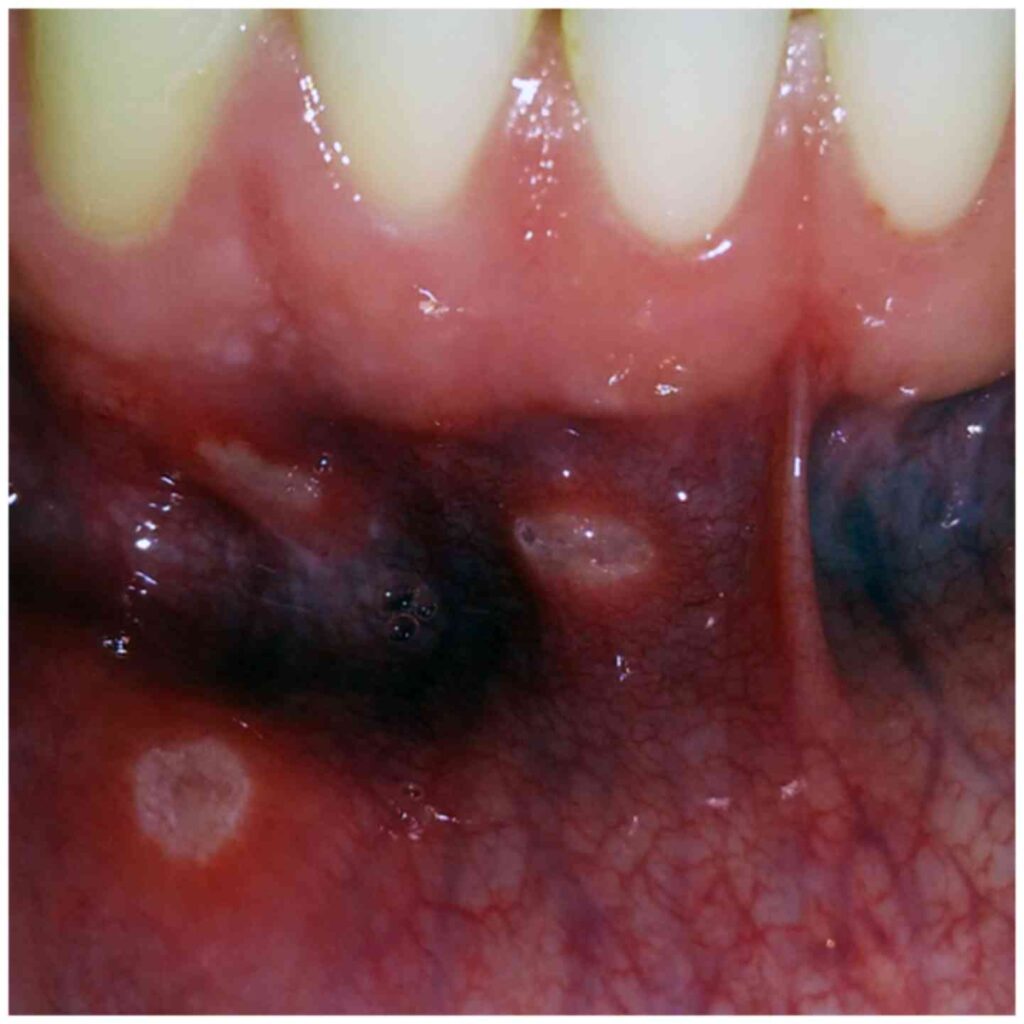
Patients typically present with:
- Round or oval ulcers with a yellow-gray base and erythematous halo
- Localized pain exacerbated by eating, drinking, and speaking
- Burning or tingling sensations preceding ulcer appearance
- Absence of systemic symptoms unless associated with systemic disease
Lesions are predominantly located on the labial and buccal mucosa, ventral tongue, soft palate, and floor of the mouth.
Diagnostic Approach to Recurrent Aphthous Stomatitis
Diagnosis is clinical, based on patient history and characteristic ulcer appearance. Additional investigations may be necessary in atypical cases or when systemic disease is suspected:
- Blood Tests:
- Complete blood count
- Iron studies
- Vitamin B12 and folate levels
- Celiac serology
- Biopsy:
- Indicated for persistent, atypical, or suspicious lesions to exclude malignancy or infectious etiologies.
- Systemic Disease Screening:
- Assessment for gastrointestinal disorders, Behçet’s disease, or immunodeficiency.
Timely and accurate diagnosis is essential to exclude other serious oral pathologies.
Management and Treatment Strategies for Recurrent Aphthous Stomatitis
While there is no definitive cure for RAS, treatment focuses on symptom relief, reduction in ulcer frequency, and promotion of healing:
Topical Therapies
- Corticosteroids:
- First-line therapy (e.g., triamcinolone acetonide, clobetasol gel)
- Antiseptic Mouthwashes:
- Chlorhexidine gluconate to prevent secondary infections
- Topical Analgesics:
- Lidocaine gel for pain control
- Protective Pastes:
- Barrier formulations to shield ulcers from irritation
Systemic Therapies
Reserved for severe, frequent, or refractory cases:
- Oral corticosteroids (e.g., prednisone)
- Immunomodulators (e.g., colchicine, dapsone, thalidomide)
- Nutritional supplementation where deficiencies are identified
Preventive Measures and Lifestyle Modifications
Proactive strategies can minimize the recurrence and severity of aphthous ulcers:
- Avoidance of known food triggers and allergens
- Stress management through behavioral therapy or relaxation techniques
- Meticulous oral hygiene using non-irritating toothpaste (e.g., SLS-free formulations)
- Correction of nutritional deficiencies
- Protection against local trauma with orthodontic wax or dental guards
Maintaining optimal systemic health is vital to reducing RAS episodes.
Differential Diagnosis of Recurrent Oral Ulcers
Several conditions may mimic RAS and should be differentiated carefully:
| Condition | Distinguishing Features |
|---|---|
| Herpes Simplex Virus | Initial vesicles, systemic symptoms |
| Behçet’s Disease | Genital ulcers, ocular involvement |
| Celiac Disease | Associated with gastrointestinal symptoms |
| Crohn’s Disease | Granulomatous inflammation, GI tract ulcers |
| Oral Lichen Planus | Lacy white striations (Wickham’s striae) |
| Pemphigus Vulgaris | Blistering lesions on mucosa and skin |
Precise diagnosis ensures appropriate management pathways are followed.
Recurrent aphthous stomatitis is a prevalent and challenging oral condition with a complex, multifactorial etiology. Through comprehensive evaluation, individualized treatment, and preventive strategies, we can significantly alleviate patient discomfort and improve quality of life. Persistent research into its immunopathogenesis holds promise for future targeted therapies.