Pure red cell aplasia (PRCA) is a rare hematologic disorder characterized by a severe reduction or complete absence of erythroid precursors in the bone marrow, while other hematopoietic lineages remain unaffected. The resulting effect is a profound normocytic, normochromic anemia accompanied by reticulocytopenia, in the absence of leukopenia or thrombocytopenia.
PRCA may manifest as either a congenital or acquired condition, with the latter more commonly associated with autoimmune diseases, infections, thymic neoplasms, hematologic malignancies, and exposure to certain medications.
Pathophysiology and Etiological Classification
The hallmark of PRCA is selective inhibition of erythropoiesis. The mechanisms may involve direct immune-mediated destruction of erythroid precursors, antibody-mediated inhibition of erythropoietin (EPO), or viral cytotoxicity.
Etiologic Classification of PRCA
| Type | Subtype | Common Causes |
|---|---|---|
| Congenital PRCA | Diamond-Blackfan Anemia | Ribosomal protein gene mutations |
| Acquired PRCA | Primary (Idiopathic) | Autoimmune origin |
| Secondary | Thymoma, viral infections (parvovirus B19), hematologic malignancies, autoimmune diseases, drugs |
Clinical Manifestations and Patient Presentation
The clinical picture is largely driven by the severity of anemia. Symptoms are usually insidious unless PRCA develops acutely.
Common Symptoms:
- Fatigue and weakness
- Pallor
- Dyspnea on exertion
- Tachycardia
- Dizziness or light-headedness
- Exertional intolerance
In cases associated with thymoma or lymphoproliferative disorders, additional systemic signs may be present.
Diagnostic Criteria and Investigative Workup
Essential Laboratory Findings
- Complete Blood Count (CBC): Isolated normocytic, normochromic anemia with very low reticulocyte count.
- Reticulocyte Count: Reticulocytopenia (<1%)
- Peripheral Blood Smear: Absence of polychromasia; normal leukocyte and platelet morphology.
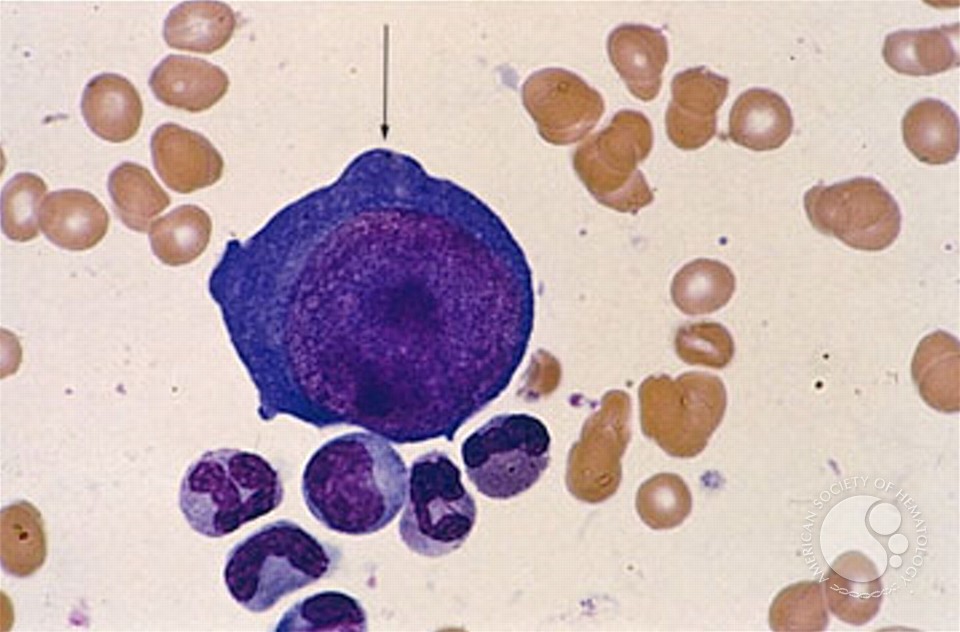
- Bone Marrow Biopsy: Profound absence of erythroid precursors with preserved myeloid and megakaryocytic lineages.
Differential Diagnosis of Pure Red Cell Aplasia
A methodical exclusion of other causes of anemia is critical in confirming PRCA.
| Condition | Distinguishing Features |
|---|---|
| Aplastic Anemia | Pancytopenia affecting all cell lines |
| Myelodysplastic Syndrome | Dysplastic changes in bone marrow and blood |
| Iron Deficiency Anemia | Microcytic anemia with elevated RDW |
| Hemolytic Anemia | Elevated reticulocyte count, indirect bilirubin, LDH |
Management and Therapeutic Approaches
The treatment of PRCA hinges on its underlying etiology. In idiopathic cases, immunosuppressive therapy forms the cornerstone of management.
Treatment by Etiology
| Cause | Management |
|---|---|
| Idiopathic/Autoimmune | Corticosteroids (e.g., prednisone), cyclosporine, cyclophosphamide |
| Thymoma-Associated | Surgical thymectomy ± immunosuppression |
| Parvovirus B19 | IVIG therapy, especially in immunocompromised patients |
| Drug-Induced | Withdrawal of offending agent |
| Lymphoproliferative Disorders | Treat underlying malignancy |
Second-Line Options
- Rituximab for B-cell–mediated autoimmune PRCA
- Anti-thymocyte globulin (ATG) for refractory cases
- Erythropoiesis-stimulating agents if EPO deficiency coexists
- Bone marrow transplantation in select congenital cases
Monitoring, Prognosis, and Long-Term Outlook
Long-term follow-up is essential to monitor for relapse and assess response to therapy. Patients treated for thymoma-associated PRCA may achieve durable remission post-thymectomy. In contrast, autoimmune or idiopathic PRCA may require prolonged immunosuppression.
Monitoring Parameters
- Hemoglobin and reticulocyte levels
- Bone marrow reassessment if relapse suspected
- Surveillance imaging if associated with malignancy
Pure red cell aplasia is a rare but significant cause of chronic anemia that necessitates prompt recognition and targeted management. With advances in immunosuppressive therapies and improved diagnostic algorithms, most patients can achieve meaningful hematologic recovery. A structured approach to evaluation and individualized treatment strategies remains vital in optimizing outcomes in both congenital and acquired forms of PRCA.