Proteus cystitis represents a significant form of urinary tract infection (UTI) caused predominantly by Proteus mirabilis, a motile, gram-negative bacterium within the Enterobacteriaceae family. Known for its urease activity and propensity to form biofilms and urinary stones, Proteus species are especially concerning in patients with indwelling catheters or recurrent infections. Accurate recognition and effective treatment of this condition are critical to preventing long-term urological complications.
Etiology and Pathophysiology of Proteus Cystitis
Proteus mirabilis is the most common species implicated in cystitis. It is capable of colonizing the urinary tract through ascending infection, often facilitated by catheterization or urinary stasis.
Pathogenic Mechanisms
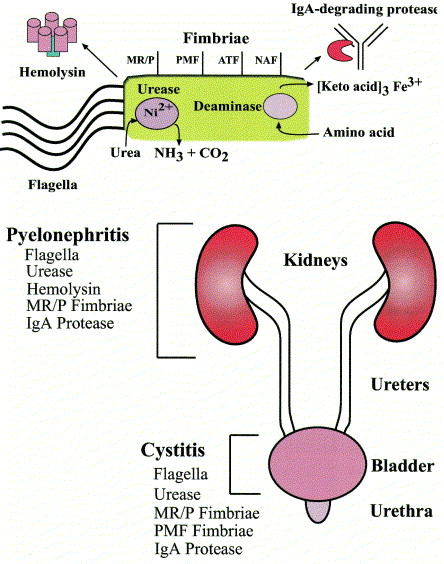
- Urease production: Hydrolyzes urea into ammonia and carbon dioxide, alkalinizing urine and promoting struvite stone formation.
- Flagella-mediated motility: Enhances ascent through the urethra.
- Fimbriae adhesion: Facilitates attachment to uroepithelial cells.
- Biofilm formation: Promotes chronic infection and resistance to antibiotics.
These virulence factors collectively contribute to persistent and recurrent infections, often with complications such as pyelonephritis or urolithiasis.
Risk Factors for Proteus-Associated UTIs
While Proteus infections may occur in otherwise healthy individuals, several conditions predispose patients to more severe or recurrent episodes:
- Prolonged indwelling catheter use
- Urinary retention or obstruction (e.g., BPH)
- Neurogenic bladder
- Structural abnormalities of the urinary tract
- History of urinary calculi
- Immunosuppression or diabetes mellitus
- Prior antibiotic exposure disrupting normal flora
Clinical Manifestations of Proteus Cystitis
Symptoms of Proteus cystitis largely mirror those of typical lower urinary tract infections but may be exacerbated by stone formation or underlying urological abnormalities.
Common Clinical Features
- Dysuria (burning urination)
- Urinary urgency and frequency
- Suprapubic pain or discomfort
- Cloudy, malodorous urine
- Hematuria (visible or microscopic)
- Fever and flank pain in upper tract involvement
Diagnostic Evaluation and Laboratory Workup
A thorough diagnostic approach is essential to confirm the etiology and tailor appropriate antimicrobial therapy.
Urine Culture Interpretation
- Proteus mirabilis is typically found in significant colony counts (>10⁵ CFU/mL).
- Alkaline urine pH is frequently observed due to urease activity.
Imaging Studies
Indicated when:
- Recurrent infections are present
- Symptoms suggest upper urinary tract involvement
- Stones or obstruction are suspected
Antimicrobial Treatment Strategies
Proteus species exhibit intrinsic resistance to certain antibiotics, such as nitrofurantoin and tetracyclines. Culture-guided therapy is preferred.
First-Line Treatment Options
- Trimethoprim-sulfamethoxazole
- Ciprofloxacin or levofloxacin
- Amoxicillin-clavulanate
- Third-generation cephalosporins (e.g., cefixime, ceftriaxone)
Duration of Therapy
- Uncomplicated cystitis: 7–10 days
- Complicated or recurrent cystitis: 10–14 days
- With urinary calculi or catheter: Extended treatment plus source control
Adjunctive Management
- Catheter removal or replacement
- Stone removal or urological intervention
- Hydration and bladder flushing to reduce bacterial load
Recurrent Proteus Cystitis: Prevention and Long-Term Management
Preventing recurrent episodes is critical for patients with chronic or complicated UTIs due to Proteus.
Preventive Measures
- Regular catheter care or intermittent catheterization
- Management of bladder emptying issues
- Prophylactic antibiotics in select cases
- Surgical correction of anatomical defects
- Monitoring for and removing urinary stones
Monitoring and Follow-Up
- Repeat urine cultures post-treatment
- Imaging for stone recurrence
- Assessment for asymptomatic bacteriuria in high-risk groups
Complications of Untreated Proteus Cystitis
Delayed or inappropriate management can lead to serious complications:
- Pyelonephritis
- Renal abscess
- Sepsis
- Bladder or kidney stone formation
- Chronic bacteriuria
Timely diagnosis and treatment are therefore imperative, particularly in vulnerable populations.
Proteus cystitis is a clinically important and potentially recurrent urinary tract infection, particularly in catheterized or anatomically compromised patients. The organism’s ability to alkalinize urine and promote stone formation complicates treatment and necessitates tailored antibiotic therapy, combined with preventative strategies and vigilant monitoring. Understanding the microbiological behavior of Proteus species and adopting a multidisciplinary approach ensures effective control and prevents recurrence or progression to severe urological disease.