Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), remains a significant global health concern due to its high recurrence rate and potential for fatal outcomes. The risk of recurrence persists long after the initial event, necessitating a structured and personalized approach to secondary prevention. This article outlines the most effective clinical strategies for the prevention of venous thromboembolism recurrence, supported by current guidelines and evidence-based practices.
Understanding the Risk of Recurrent Venous Thromboembolism
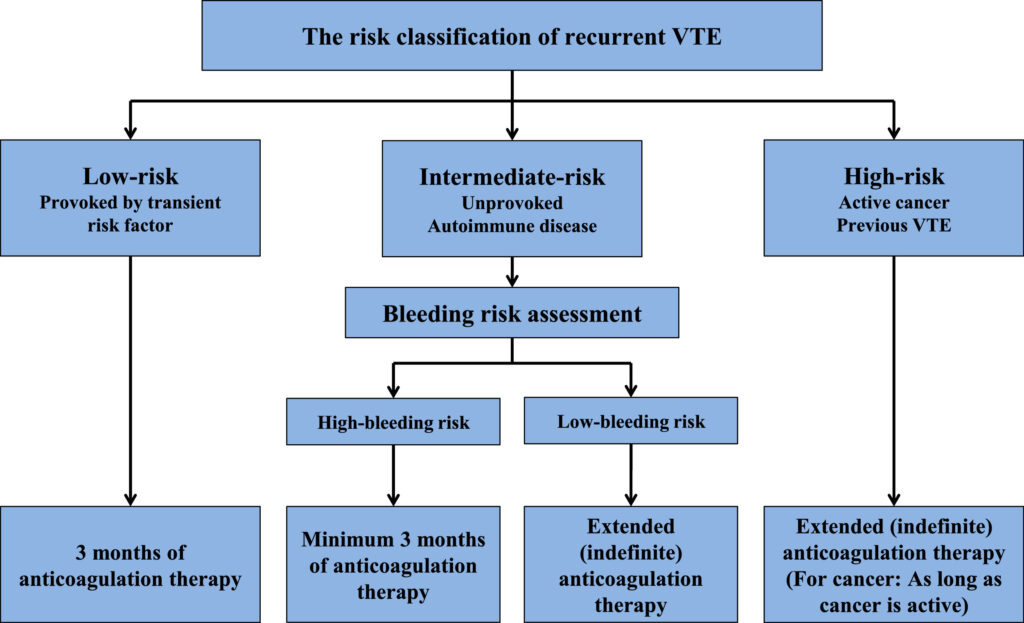
Classification of VTE Events
- Provoked VTE: Triggered by transient risk factors such as surgery, trauma, or prolonged immobility.
- Unprovoked VTE: Occurs in the absence of identifiable risk factors and carries a higher risk of recurrence.
- Cancer-Associated Thrombosis: VTE in the context of malignancy is associated with both higher recurrence and bleeding risks.
Key Risk Factors for Recurrence
- Male sex
- Elevated D-dimer after cessation of therapy
- Obesity (BMI >30)
- Persistent antiphospholipid antibodies
- Active malignancy
- Previous unprovoked VTE
- Genetic thrombophilias (e.g., Factor V Leiden)
Stratification and Risk Assessment Tools
Determining the Duration of Anticoagulation
Individualized risk-benefit analysis is critical. Risk stratification tools help guide the decision to extend anticoagulation beyond the initial 3 to 6 months.
Recommended Tools:
- HERDOO2 Rule: For identifying low-risk women for discontinuation.
- Vienna Prediction Model
- DASH Score: D-dimer, Age, Sex, Hormone therapy
Long-Term Anticoagulation Therapy for Recurrence Prevention
Direct Oral Anticoagulants (DOACs)
DOACs such as apixaban, rivaroxaban, edoxaban, and dabigatran are preferred for long-term secondary prevention due to favorable safety profiles.
Recommended Regimens:
- Apixaban: 2.5 mg BID for extended therapy
- Rivaroxaban: 10 mg OD after initial 6 months
Vitamin K Antagonists (Warfarin)
Still effective, especially for patients with mechanical valves or antiphospholipid syndrome. INR must be maintained between 2.0 and 3.0.
Low Molecular Weight Heparin (LMWH)
First-line for patients with cancer-associated thrombosis (e.g., dalteparin, enoxaparin), though DOACs are increasingly used with caution.
Tailoring Therapy: Duration and Intensity
Short-Term Therapy (3–6 Months)
Indicated for provoked VTE with transient risk factors. Low recurrence risk post-therapy.
Extended Therapy (Indefinite)
Recommended for:
- Unprovoked proximal DVT or PE
- Recurrent VTE
- Active cancer
- High-risk thrombophilias
Regular reevaluation of bleeding risk is mandatory during extended therapy.
Non-Pharmacologic Strategies and Lifestyle Modifications
Compression Therapy
- Graduated compression stockings can reduce post-thrombotic syndrome but do not lower recurrence risk.
- Used for symptom management in patients with chronic venous insufficiency.
Physical Activity and Weight Management
- Encouraged to reduce risk of recurrent VTE
- Avoid prolonged immobility, especially during travel
Smoking Cessation and Alcohol Moderation
- Reduces overall cardiovascular risk and supports effective anticoagulation control
Monitoring and Follow-Up Protocols
D-Dimer Testing Post-Anticoagulation
Elevated D-dimer levels 3–4 weeks after cessation of anticoagulation can identify patients at increased risk of recurrence and guide decisions on extended therapy.
Surveillance in High-Risk Groups
- Regular imaging not routinely recommended
- Focus on clinical vigilance for signs of recurrence
- Continued cancer screening in patients with unprovoked VTE
Special Populations and Considerations
Pregnancy-Associated VTE
- LMWH is the anticoagulant of choice
- Anticoagulation continued throughout pregnancy and 6 weeks postpartum
Elderly Patients
- Assess bleeding risk with tools like HAS-BLED
- DOACs preferred for ease of use and lower intracranial bleeding risk
Antiphospholipid Syndrome
- High risk of recurrence
- Warfarin preferred over DOACs
- INR goal often >2.5 depending on history
Guidelines and Recommendations from Major Societies
- American College of Chest Physicians (ACCP): Recommends at least 3 months of anticoagulation; extended therapy for unprovoked events if bleeding risk is low.
- European Society of Cardiology (ESC): Emphasizes individualized approach with periodic reassessment.
- National Comprehensive Cancer Network (NCCN): LMWH or DOACs for cancer patients with VTE.
Preventing venous thromboembolism recurrence requires a multidimensional approach incorporating individualized risk assessment, tailored duration of anticoagulation therapy, lifestyle optimization, and vigilant monitoring. By combining pharmacological and non-pharmacological strategies and adhering to evidence-based protocols, we can significantly reduce the burden of recurrent VTE and enhance patient outcomes.