Radiation-induced nausea and vomiting (RINV) is a frequent and distressing side effect experienced by cancer patients receiving radiotherapy, particularly in the abdominal and pelvic regions. RINV not only compromises patient quality of life but may also lead to non-compliance, treatment delays, and nutritional deficiencies. The severity of symptoms is influenced by radiation field size, dose, fractionation, and individual susceptibility.
Classifying RINV by Risk Potential
The likelihood of developing RINV varies by the anatomical site exposed to radiation. The classification system guides prophylactic antiemetic strategies.
| Radiation Site | RINV Risk Level |
|---|---|
| Total Body Irradiation | High |
| Upper Abdomen | Moderate to High |
| Craniospinal Irradiation | Moderate |
| Lower Thorax, Pelvis | Low to Moderate |
| Extremities, Head & Neck | Minimal |
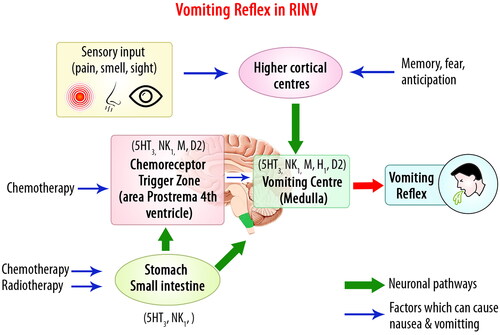
Mechanism of Nausea and Vomiting in Radiation Therapy
Radiation stimulates the chemoreceptor trigger zone (CTZ) and gastrointestinal tract, leading to the release of:
- Serotonin (5-HT3) from enterochromaffin cells
- Substance P acting on neurokinin-1 (NK1) receptors
- Dopamine and other neurotransmitters contributing to the emetic reflex
Patient-Related Risk Factors
- Female gender
- Age <55 years
- History of motion sickness or morning sickness
- Prior chemotherapy-induced nausea
- Anxiety or psychological distress
Core Strategy: Prophylactic Antiemetic Therapy
1. 5-HT3 Receptor Antagonists
These agents block serotonin at both central and peripheral receptors.
Recommended drugs:
- Ondansetron
- Granisetron
- Palonosetron
Dosage example:
- Ondansetron 8 mg orally 30–60 minutes before radiotherapy, continued once daily
2. NK1 Receptor Antagonists
Used for moderate-to-high risk RINV when combined with 5-HT3 antagonists.
Example:
- Aprepitant 125 mg on day 1, 80 mg on subsequent days
3. Corticosteroids
Steroids enhance antiemetic efficacy of both 5-HT3 and NK1 agents.
Dexamethasone dosing:
- 4–8 mg orally before radiation, then 4 mg daily for 2–3 days
Combination Antiemetic Regimens by Risk Level
| RINV Risk Category | Prophylactic Regimen |
|---|---|
| High | 5-HT3 + NK1 + Dexamethasone |
| Moderate | 5-HT3 ± Dexamethasone |
| Low | Dexamethasone or 5-HT3 |
| Minimal | No routine prophylaxis; rescue therapy if needed |
Non-Pharmacological Interventions for RINV Prevention
1. Dietary Modifications
- Small, frequent meals
- Avoidance of greasy, spicy, or strong-smelling foods
- Bland, cold, or room-temperature meals
2. Acupressure and Acupuncture
Stimulation of P6 (Neiguan) point may reduce nausea through vagal modulation.
3. Psychological Support
Cognitive-behavioral therapy and guided imagery techniques help reduce anticipatory nausea, which often precedes actual emesis.
Personalized Approach to RINV Management
Tailoring prevention strategies to individual patient profiles enhances efficacy and tolerability.
Considerations include:
- Past antiemetic response
- Patient preferences
- Comorbid conditions (e.g., diabetes, peptic ulcer)
- Drug-drug interactions
Monitoring and Follow-Up Protocol
Regular assessment allows early intervention and avoids symptom escalation.
Recommended Assessment Tools:
- NCI-CTCAE Grading of nausea and vomiting
- Patient diaries documenting emetic episodes and triggers
- Adherence tracking for antiemetic intake
Special Considerations: Pediatric and Geriatric Populations
Pediatrics:
- Dose-adjusted antiemetics
- Greater use of non-pharmacologic interventions
- Importance of caregiver involvement
Geriatrics:
- Cautious steroid use due to comorbidities
- Monitor for QT prolongation with 5-HT3 antagonists
- Adjust doses for renal/hepatic impairment
Managing Breakthrough and Refractory RINV
Breakthrough RINV
Occurs despite prophylaxis—treat with a different class of antiemetic:
- Add dopamine antagonist (e.g., metoclopramide)
- Use benzodiazepines for anxiety-driven symptoms
Refractory RINV
Persistent symptoms—consider:
- Review of radiation field for anatomical cause
- Combination of multiple antiemetic classes
- Referral to palliative care or supportive oncology
Preventing radiation-induced nausea and vomiting demands a structured, risk-adapted, and patient-focused approach. Evidence supports the use of 5-HT3 receptor antagonists, NK1 receptor antagonists, corticosteroids, and behavioral therapies tailored to the emetogenic potential of radiotherapy. Meticulous execution of prophylactic protocols enables improved treatment adherence, reduced distress, and enhanced quality of life for oncology patients.