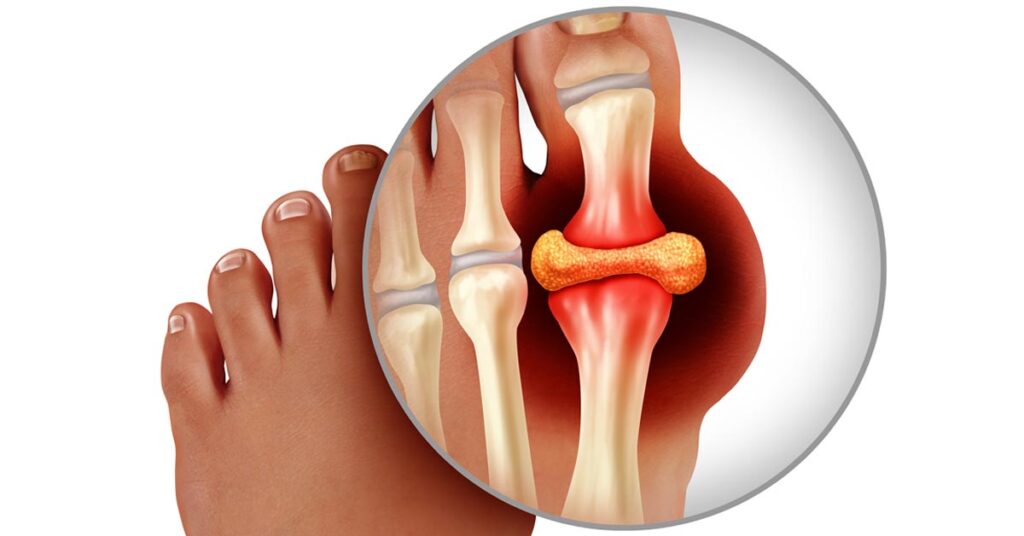
Acute gout attacks are intensely painful episodes of joint inflammation caused by the crystallization of monosodium urate in synovial fluid. While treatment is vital during an active flare, long-term prevention is essential to reduce recurrence, joint damage, and systemic complications. Effective prevention strategies encompass pharmacologic interventions, lifestyle modifications, and dietary management targeted at controlling serum uric acid levels and minimizing trigger exposure.
Understanding Acute Gout Attacks and Risk Factors
Acute gout is triggered when serum urate levels exceed the solubility threshold, typically above 6.8 mg/dL, leading to crystal deposition, immune activation, and inflammation. Certain factors increase the risk of flares:
- Hyperuricemia (elevated serum uric acid)
- Alcohol consumption (especially beer and spirits)
- High-purine diet (red meat, organ meats, shellfish)
- Dehydration or rapid fluid shifts
- Use of diuretics, aspirin, cyclosporine
- Sudden initiation or discontinuation of urate-lowering therapy
Identifying and managing these risk factors is central to preventing acute episodes.
Initiating Long-Term Uric Acid-Lowering Therapy
For individuals with recurrent flares, tophi, chronic kidney disease, or urate nephrolithiasis, urate-lowering therapy (ULT) is indicated.
First-Line Urate-Lowering Medications
- Allopurinol: Xanthine oxidase inhibitor; initial dose 100 mg/day, titrated to maintain urate <6.0 mg/dL
- Febuxostat: Alternative xanthine oxidase inhibitor, used in cases of allopurinol intolerance
- Probenecid: Uricosuric agent that increases renal uric acid excretion (less effective in renal impairment)
Allopurinol remains the gold standard due to efficacy, safety, and cost-effectiveness.
Timing and Precautions
ULT should not be started during an active flare. Initiation during quiescence with prophylactic anti-inflammatory coverage reduces risk of triggering new attacks.
Anti-Inflammatory Prophylaxis During ULT Initiation
To mitigate the risk of flares during early urate-lowering therapy, prophylactic anti-inflammatory agents are recommended for 3–6 months.
Recommended Prophylaxis Options
- Colchicine: 0.6 mg once or twice daily
- NSAIDs: Naproxen 250 mg twice daily (if no contraindications)
- Low-dose corticosteroids: Prednisone 5–10 mg daily (in NSAID/colchicine intolerance)
Regular monitoring is advised, particularly in older adults or those with renal/hepatic impairment.
Dietary Management: Reducing Purine Intake and Metabolic Risk
A tailored diet plays a critical role in managing serum uric acid and reducing gout attacks.
Gout-Friendly Dietary Guidelines
- Limit high-purine foods: Red meats, organ meats, anchovies, sardines
- Avoid sugary beverages and fructose-rich food: Linked to increased uric acid production
- Moderate alcohol intake: Beer and spirits are high-risk; wine is comparatively safer
- Increase low-fat dairy products: May lower uric acid levels
- Consume complex carbs and whole grains
- Stay hydrated: Encourages uric acid excretion through urine
Adopting a DASH-style diet or Mediterranean diet may also support cardiovascular health in gout patients.
Weight Management and Physical Activity
Obesity is a major contributor to hyperuricemia and gout flares. Sustainable weight loss through caloric control and exercise significantly lowers urate levels.
- Target a gradual weight loss of 1–2 pounds per week
- Avoid crash diets or fasting, which can precipitate flares
- Engage in moderate-intensity aerobic activity 150 minutes per week
- Incorporate resistance training twice weekly for joint health
Reducing visceral fat also improves insulin sensitivity, further aiding urate control.
Managing Comorbidities: A Holistic Approach to Gout Prevention
Gout is often associated with a cluster of metabolic and cardiovascular conditions:
- Hypertension
- Type 2 Diabetes Mellitus
- Chronic kidney disease
- Hyperlipidemia
Effective management of these comorbidities through medications and lifestyle adjustments enhances uric acid control and reduces overall flare risk.
- Use losartan or calcium channel blockers for hypertensive patients (uricosuric effect)
- Avoid thiazide and loop diuretics if possible
- Optimize renal function through hydration and nephroprotective agents
Adherence and Patient Education: A Key Component of Prevention
Long-term prevention depends on patient adherence and understanding of gout’s chronic nature.
- Educate patients that ULT is lifelong and not discontinued after symptom relief
- Reinforce adherence through regular follow-ups and uric acid monitoring
- Use visual aids or mobile apps to track diet, medications, and urate levels
- Encourage family involvement for lifestyle changes
Informed patients are more likely to comply with therapy and reduce future flares.
Avoiding Common Gout Triggers
Trigger identification is unique to each individual. Patients should:
- Keep a symptom diary to identify food or stress-related triggers
- Avoid excessive exercise or trauma to joints, especially in those with a history of flares
- Monitor medication side effects or interactions that could elevate urate levels
Preventive care must be personalized and proactive.
Preventing acute gout attacks requires an integrated approach—long-term urate lowering therapy, flare prophylaxis, dietary modifications, weight management, and comorbidity control. With sustained adherence and lifestyle restructuring, the burden of painful flares and joint destruction can be significantly reduced, leading to improved quality of life.