Peyronie’s disease is a noncancerous condition characterized by the development of fibrous scar tissue, or plaque, within the penis. This leads to abnormal curvature during erections, which may result in pain, erectile dysfunction, and significant psychological distress. While the exact prevalence is unclear due to underreporting, studies estimate that Peyronie’s disease affects approximately 1 in 11 men, primarily between the ages of 40 and 70.
Causes and Risk Factors
Collagen Buildup and Plaque Formation
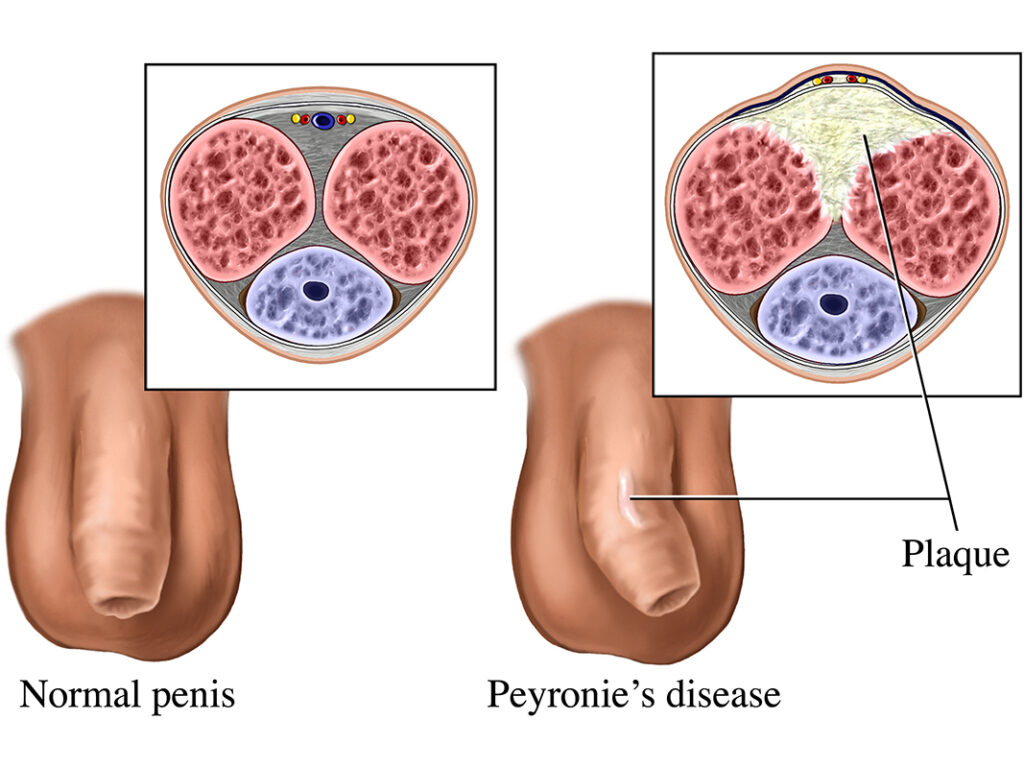
The hallmark of Peyronie’s disease is the formation of fibrous plaques made of collagen. These plaques develop inside the tunica albuginea, a thick sheath surrounding the corpora cavernosa—the two sponge-like regions that fill with blood during an erection.
Primary Triggers
- Penile Trauma: A common trigger involves repetitive minor trauma during intercourse or injury. The healing process can lead to collagen overproduction, resulting in scar tissue.
- Genetic Predisposition: Men with Dupuytren’s contracture or a family history of connective tissue disorders have a higher risk.
- Age-Related Changes: Aging contributes to reduced tissue elasticity, making injuries more likely and healing less efficient.
- Autoimmune Reactions: In some cases, the immune system mistakenly attacks healthy tissue, leading to inflammation and fibrosis.
Symptoms and Clinical Presentation
Common Signs and Manifestations
- Penile Curvature: Most noticeable during an erection; may curve upward, downward, or to the side.
- Painful Erections: Discomfort or sharp pain may occur, particularly in the acute phase.
- Erectile Dysfunction (ED): A significant proportion of affected individuals experience difficulty achieving or maintaining erections.
- Penile Shortening or Deformity: The affected region may not expand properly, causing a dent, hourglass narrowing, or visible asymmetry.
- Palpable Lumps: The plaque is often detectable as a firm area beneath the skin.
Disease Phases
- Acute Phase (6–18 months): Characterized by evolving curvature, pain, and inflammation.
- Chronic Phase: Pain generally subsides, but deformity and dysfunction persist or stabilize.
Diagnostic Evaluation
Medical History and Physical Examination
A thorough history and physical examination are critical. Physicians assess:
- Pain onset and duration
- Degree and direction of curvature
- Erectile function
- Presence of plaques via palpation
Imaging and Measurement Tools
- Penile Ultrasound: Identifies plaques, calcifications, and blood flow abnormalities.
- Erection-Induced Imaging: An artificial erection using medication may be used for curvature measurement.
- 3D Imaging Systems: Some clinics offer advanced modeling to aid in surgical planning.
Treatment Options for Peyronie’s Disease
Non-Surgical Management
1. Oral Medications (Limited Efficacy)
- Potassium para-aminobenzoate (Potaba)
- Vitamin E and L-carnitine
- Pentoxifylline: May reduce inflammation and slow plaque growth
2. Intralesional Injections
- Collagenase Clostridium Histolyticum (Xiaflex®): FDA-approved; breaks down collagen in plaques
- Verapamil: A calcium channel blocker that improves elasticity
- Interferon-alpha-2b: Reduces inflammation and plaque size
3. Traction Therapy
- Penile Traction Devices: Apply constant, gentle pressure to gradually straighten the penis; highly effective in early-stage disease.
4. Shockwave Therapy
- Low-intensity shockwaves may reduce pain and improve blood flow but are not proven to correct curvature.
Surgical Intervention
Surgery is typically reserved for severe deformity or when non-invasive treatments fail. Procedures include:
Tunica Shortening Procedures
- Nesbit Procedure or Plication: Removes or tucks tunica tissue on the opposite side of the plaque. Suitable for mild curvature.
Tunica Lengthening Procedures
- Plaque Incision with Grafting (PIG): The plaque is incised, and a graft is inserted to fill the gap. Recommended for more severe cases.
Penile Prosthesis Implantation
- Best suited for patients with significant ED and curvature. The implant allows both rigidity and straightening.
Mental Health and Emotional Support
Peyronie’s disease often causes psychological distress. Depression, anxiety, and diminished self-esteem are common. Professional counseling and support groups can provide essential coping tools and improve quality of life.
Preventive Measures and Lifestyle Modifications
While Peyronie’s disease cannot always be prevented, the following practices may reduce risk:
- Use adequate lubrication during intercourse
- Avoid aggressive sexual positions that may cause trauma
- Manage diabetes and cardiovascular conditions
- Refrain from tobacco use, which impairs vascular and tissue health
Prognosis and Outlook
While spontaneous resolution occurs in some mild cases, most men will experience stable or progressive curvature without treatment. Early intervention during the acute phase may reduce long-term deformity and dysfunction. With modern therapies, the majority of patients can regain satisfactory sexual function.
Frequently Asked Questions:
What is the main cause of Peyronie’s disease?
The primary cause is repetitive trauma to the penis, often during intercourse, which leads to abnormal collagen deposition and scar tissue formation.
Is Peyronie’s disease reversible?
Mild cases may resolve spontaneously. Others require medical or surgical treatment to improve curvature and function.
How effective is collagenase injection therapy?
Clinical trials show a significant reduction in curvature (up to 35%) in properly selected patients.
Does Peyronie’s disease affect fertility?
No, it does not affect sperm production or fertility directly, but it may hinder the ability to have intercourse.
When should I see a urologist?
If you experience noticeable curvature, painful erections, or difficulty with sexual performance, consult a urologist promptly
Peyronie’s disease is a complex condition with significant physical and emotional consequences. Early diagnosis and a personalized treatment plan are vital for optimal outcomes. Advances in medical and surgical therapies now offer hope and restoration of function for many affected men.

