Osteopenia of prematurity (OOP), also known as metabolic bone disease of prematurity, is a condition marked by decreased bone mineral content and reduced bone strength in preterm infants. It primarily affects infants born before 32 weeks of gestation or those with very low birth weight (<1500 g), due to interrupted transplacental mineral transfer and postnatal nutritional deficits.
Pathophysiology and Bone Development in Preterm Infants
During the third trimester, fetuses accumulate approximately 80% of their total calcium and phosphorus stores. Preterm birth interrupts this critical mineral accretion phase, leading to a significant reduction in bone density. Furthermore, preterm infants often have immature kidneys, reduced gastrointestinal absorption of nutrients, and limited mobility, all of which exacerbate bone demineralization.
Risk Factors Contributing to Osteopenia of Prematurity
1. Gestational Age and Birth Weight
- Infants born before 32 weeks and weighing less than 1500 grams are at highest risk.
2. Inadequate Nutritional Intake
- Parenteral nutrition lacking adequate calcium and phosphorus.
- Delayed enteral feeding.
3. Prolonged Immobilization
- Limited mechanical stimulation reduces osteoblastic activity.
4. Medications
- Chronic use of diuretics (furosemide), corticosteroids, and caffeine impairs mineral retention.
5. Underlying Illness
- Conditions such as bronchopulmonary dysplasia, necrotizing enterocolitis, or sepsis increase nutritional demands and alter mineral metabolism.
Clinical Features of Neonatal Osteopenia
Osteopenia of prematurity often presents without overt clinical symptoms in its early stages. However, as the disease progresses, the following signs may emerge:
- Reduced limb movement
- Bone tenderness
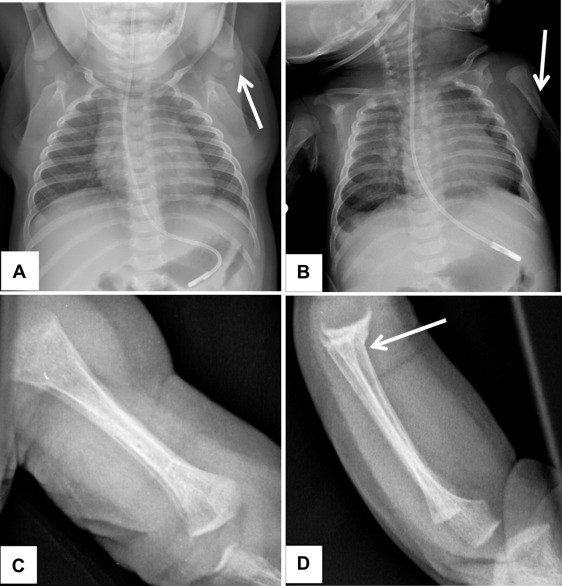
- Fractures, especially of ribs or long bones, with minimal trauma
- Craniotabes (soft skull bones)
- Delayed growth and development
Diagnostic Evaluation of Osteopenia of Prematurity
Biochemical Markers
| Test | Indicative Findings |
|---|---|
| Serum Alkaline Phosphatase (ALP) | Elevated (>800 IU/L) |
| Serum Phosphorus | Decreased (<4.5 mg/dL) |
| Serum Calcium | May be normal or low |
| Parathyroid Hormone (PTH) | Elevated in secondary hyperparathyroidism |
| 25-Hydroxyvitamin D | Indicates vitamin D stores |
Radiological Assessment
- X-rays: Reveal reduced bone density, fraying of metaphyses, and fractures.
- Quantitative Ultrasound: Non-invasive method for assessing bone mineral status.
- Dual-Energy X-ray Absorptiometry (DEXA): Gold standard for measuring bone mineral density but less accessible in neonates.
Prevention Strategies for Osteopenia in Preterm Infants
Nutritional Optimization
- Calcium: 120–220 mg/kg/day
- Phosphorus: 60–140 mg/kg/day
- Vitamin D: 400–1000 IU/day to support calcium absorption
Preferred Sources:
- Fortified human milk or preterm formulas rich in minerals
- Use of human milk fortifiers when necessary
Early Enteral Nutrition
Initiating minimal enteral feeds as early as possible reduces dependence on parenteral nutrition and supports gastrointestinal maturity, thereby improving mineral absorption.
Monitoring and Supplementation
Regular biochemical and radiological assessments guide the need for:
- Calcium and phosphorus supplementation
- Adjusting vitamin D intake
- Evaluating renal function and urinary calcium loss
Treatment of Osteopenia of Prematurity
Nutritional Management
- Adjust intake of calcium, phosphorus, and vitamin D based on monitoring.
- Transition from parenteral to enteral feeds as soon as feasible.
- Use mineral-enriched formulas if breastfeeding alone does not meet requirements.
Pharmacologic Interventions
- Phosphate supplements (oral or IV) for hypophosphatemia.
- Calcium gluconate (oral or IV) for hypocalcemia.
- Calcitriol in cases of secondary hyperparathyroidism or low 25-OH vitamin D.
Physical Activity
- Gentle physiotherapy and passive range-of-motion exercises stimulate bone formation and mineral deposition.
Prognosis and Long-Term Outcomes
With early recognition and appropriate intervention, most infants recover normal bone mineralization by term-equivalent age. However, severe or prolonged osteopenia may result in:
- Growth retardation
- Delayed motor milestones
- Increased fracture risk in infancy
Routine follow-up with pediatric endocrinology or neonatology is recommended to monitor growth and bone health beyond the neonatal period.
Frequently Asked Questions
What is osteopenia of prematurity?
A metabolic bone disorder in preterm infants characterized by reduced bone mineral content due to interrupted mineral transfer and nutritional deficits.
When is osteopenia usually detected in preterm infants?
Typically appears between 4 to 8 weeks postnatal age in infants born before 32 weeks of gestation.
Can osteopenia of prematurity be reversed?
Yes, with proper nutrition, supplementation, and monitoring, bone mineralization can normalize by term-corrected age.
What is the most sensitive biochemical marker?
Serum alkaline phosphatase is the most sensitive early indicator of impaired bone mineralization.
Are fractures common in osteopenia of prematurity?
Yes, particularly in severe cases. Ribs and long bones are most frequently affected.
Osteopenia of prematurity is a preventable and manageable condition when approached with timely intervention and a multidisciplinary strategy. Ensuring optimal mineral and vitamin D intake, along with close clinical monitoring, allows preterm infants to achieve adequate bone health and normal development. Proactive care during the neonatal period is critical in minimizing complications and supporting long-term outcomes.