Osteolytic bone metastases are a common and serious complication of advanced breast cancer. These metastases occur when malignant breast cancer cells migrate from the primary tumor site to the bone, disrupting the normal balance of bone remodeling and leading to localized bone destruction. The result is weakened skeletal structure, pain, and increased fracture risk. Among patients with metastatic breast cancer, bone is the most frequent site of distant spread, with osteolytic lesions being predominant.
Pathophysiology: Mechanism of Bone Destruction
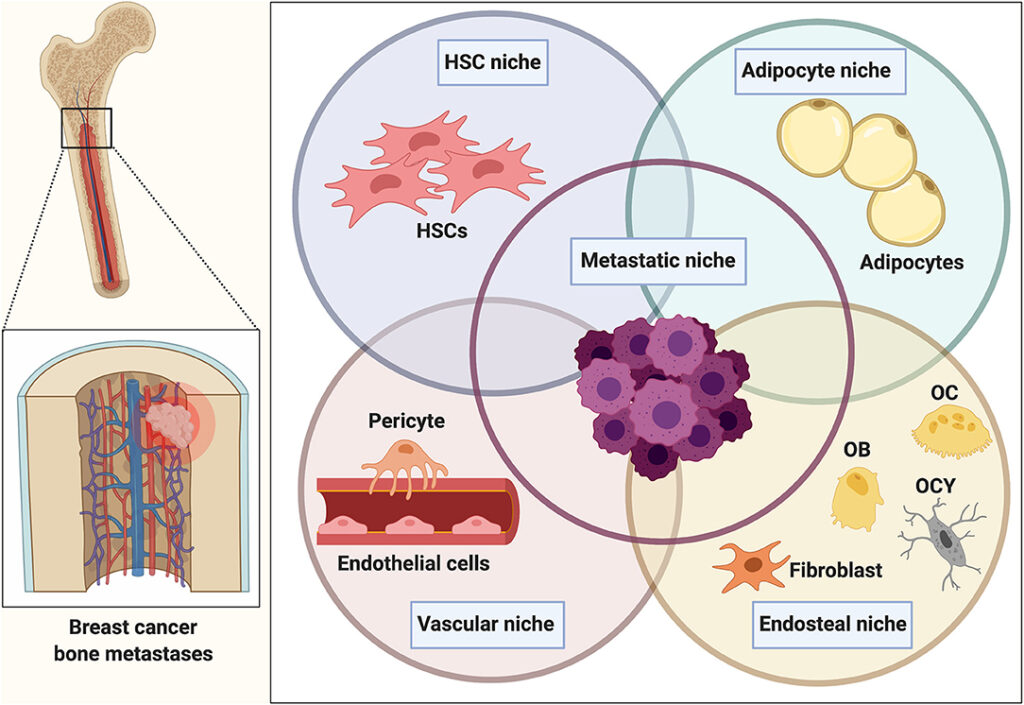
The pathogenesis of osteolytic lesions in breast cancer is driven by the interaction between tumor cells, osteoclasts, and the bone microenvironment.
Cellular Interactions
Breast cancer cells secrete various factors such as:
- Parathyroid hormone-related protein (PTHrP)
- Interleukins (IL-6, IL-11)
- Tumor necrosis factor-alpha (TNF-α)
These molecules stimulate osteoclast differentiation and activation, leading to bone resorption.
Disruption of Bone Homeostasis
Bone resorption releases growth factors (e.g., TGF-β, IGFs) embedded in the bone matrix, which in turn promote tumor growth—a vicious cycle that amplifies bone destruction.
Clinical Manifestations and Symptoms
Patients with osteolytic bone metastases may present with:
- Bone pain: Often the first and most prominent symptom
- Pathological fractures: Especially in weight-bearing bones
- Hypercalcemia of malignancy: Due to excessive bone turnover
- Spinal cord compression: From vertebral collapse or tumor expansion
- Reduced mobility and quality of life
Diagnostic Approach
Imaging Techniques
Accurate and early detection is essential for timely intervention.
- X-ray: Useful for detecting advanced lytic lesions.
- Bone Scintigraphy: Detects osteoblastic activity; may miss purely lytic lesions.
- MRI: Excellent for soft tissue involvement and spinal cord compression.
- CT Scan: Provides detailed bone architecture.
- PET-CT: Useful in evaluating the metabolic activity and extent of metastases.
Laboratory Tests
- Serum Calcium: Elevated in cases of hypercalcemia.
- Tumor Markers: CA 15-3, CEA may be elevated.
- Bone Turnover Markers: Include N-telopeptide (NTX) and C-terminal telopeptide (CTX).
Histological Confirmation
While imaging is often sufficient, a biopsy may be warranted to confirm the diagnosis, especially when:
- The lesion is solitary
- Primary cancer history is unknown
- There is suspicion of another pathology
Management of Osteolytic Bone Metastases
A multidisciplinary approach involving oncology, orthopedics, radiology, and palliative care is essential.
Systemic Cancer Therapies
- Endocrine Therapy: For hormone receptor-positive tumors.
- Chemotherapy: Especially in rapidly progressive disease.
- Targeted Therapy: HER2 inhibitors (e.g., trastuzumab) for HER2-positive tumors.
- Immunotherapy: Considered in triple-negative breast cancer cases.
Bone-Directed Treatments
- Bisphosphonates (e.g., zoledronic acid): Inhibit osteoclast-mediated bone resorption, reduce skeletal-related events (SREs).
- Denosumab: A monoclonal antibody targeting RANKL, offering superior efficacy in preventing SREs compared to bisphosphonates.
Radiotherapy
- Palliative Radiotherapy: Relieves pain and controls local disease.
- Stereotactic Body Radiotherapy (SBRT): Used for oligometastatic disease with precision targeting.
Surgical Interventions
- Prophylactic fixation: To prevent fractures in structurally compromised bones.
- Vertebroplasty/Kyphoplasty: Stabilizes vertebral fractures and alleviates pain.
- Spinal decompression: Required in cases of spinal cord compression.
Hypercalcemia Management
Hypercalcemia is a medical emergency requiring prompt treatment:
- Hydration with IV fluids
- Loop diuretics (e.g., furosemide)
- Bisphosphonates or Denosumab
- Calcitonin for rapid calcium reduction
- Dialysis in refractory cases
Prognosis and Survival
Survival in patients with bone metastases from breast cancer depends on multiple factors:
- Tumor biology and receptor status
- Response to systemic therapy
- Number and location of bone metastases
- Presence of visceral metastases
On average, patients with bone-only metastases have a better prognosis compared to those with visceral involvement. Survival may extend from several months to multiple years, particularly in hormone receptor-positive disease controlled by targeted treatments.
Complications of Bone Metastases
- Skeletal-related events (SREs): Fractures, need for radiation or surgery, spinal cord compression
- Functional impairment: Reduced independence
- Chronic pain: Requiring long-term management
- Psychological distress: Anxiety, depression, and decreased quality of life
Ongoing Research and Emerging Therapies
The landscape of metastatic breast cancer treatment is evolving with advances in:
- Bone-targeting agents: New RANKL inhibitors, cathepsin K inhibitors
- Combination therapies: Integrating immunotherapy with bone-targeted treatments
- Tumor microenvironment modulation: Inhibiting the vicious cycle of bone destruction and tumor growth
- Liquid biopsy and biomarkers: Enhancing early detection and treatment personalization
Frequently Asked Questions:
What causes osteolytic bone metastases in breast cancer?
They result from breast cancer cells stimulating osteoclasts, leading to bone breakdown.
Are osteolytic lesions painful?
Yes, bone pain is a common and early symptom due to structural weakening and nerve involvement.
How are bone metastases from breast cancer diagnosed?
Through a combination of imaging, lab tests, and sometimes biopsy.
Can bone metastases be cured?
They are usually not curable but can be managed effectively to improve quality of life and survival.
What is the best treatment for bone metastases?
A combination of systemic cancer therapy and bone-directed treatments like bisphosphonates or denosumab.
Osteolytic bone metastases represent a significant clinical challenge in the management of advanced breast cancer. Effective diagnosis, timely intervention, and a personalized treatment plan are critical for preserving skeletal integrity, minimizing complications, and enhancing patient outcomes. With continued advancements in both systemic and bone-targeted therapies, the prognosis and quality of life for affected individuals continue to improve.