Ocular Surface Squamous Neoplasia (OSSN) encompasses a spectrum of dysplastic and neoplastic lesions of the conjunctiva and cornea, ranging from mild epithelial dysplasia to invasive squamous cell carcinoma. OSSN is the most common non-pigmented malignancy of the ocular surface and is increasingly diagnosed globally due to improved clinical awareness and diagnostic tools.
Epidemiology and Risk Factors
OSSN has a variable global distribution, with higher incidence rates reported in regions with elevated ultraviolet (UV) radiation exposure, particularly in equatorial Africa and Australia.
Key Risk Factors:
- Ultraviolet B radiation (UVB) exposure
- Human papillomavirus (HPV) infection, especially HPV-16 and 18
- HIV/AIDS and immunosuppression
- Older age, typically over 60 years
- Fair skin and light eye color
- Chronic ocular surface inflammation
- Exposure to petroleum-based products
Pathogenesis of OSSN
The development of OSSN is multifactorial, involving genetic mutations, viral oncogenes, and environmental damage. UVB radiation induces mutations in the p53 tumor suppressor gene, leading to uncontrolled epithelial proliferation. In immunocompromised patients, HPV oncoproteins disrupt cell cycle regulation, further accelerating neoplastic transformation.
Clinical Presentation and Signs
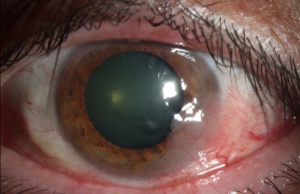
OSSN typically presents as a unilateral, elevated, gelatinous, or leukoplakic lesion at the limbus, often on the nasal side. Lesions can range from small, localized patches to large, invasive masses.
Common Symptoms:
- Redness and ocular irritation
- Foreign body sensation
- Decreased vision (in advanced cases)
- Visible mass on conjunctiva or cornea
- Recurrent conjunctivitis-like appearance
Classification of OSSN
OSSN is categorized histologically based on the degree of epithelial involvement:
- Conjunctival Intraepithelial Neoplasia (CIN):
- CIN I: mild dysplasia
- CIN II: moderate dysplasia
- CIN III: severe dysplasia/carcinoma in situ
- Invasive Squamous Cell Carcinoma (SCC):
- Tumor breaches the basement membrane and invades underlying stroma
Diagnostic Techniques for OSSN
Timely diagnosis is critical for successful management of OSSN. Clinical suspicion must be confirmed through a combination of non-invasive and invasive techniques.
Slit-Lamp Examination:
- Observes lesion features such as feeder vessels, keratinization, and leukoplakia
- Fluorescein staining to evaluate epithelial irregularity
Impression Cytology:
- Non-invasive method that collects surface cells for cytological analysis
- Helpful for detecting dysplasia and confirming OSSN diagnosis
In Vivo Confocal Microscopy (IVCM):
- High-resolution imaging of ocular tissues
- Reveals hyper-reflective, irregular epithelial cells and mitotic figures
Anterior Segment Optical Coherence Tomography (AS-OCT):
- Delineates lesion depth and epithelial thickening
- Differentiates OSSN from benign lesions like pterygium
Histopathology (Gold Standard):
- Surgical excision followed by histological evaluation
- Determines degree of dysplasia and invasion
Treatment Modalities for OSSN
Treatment of OSSN is determined by the lesion’s size, location, degree of invasion, and patient-specific factors such as immune status.
Surgical Management
Excisional Biopsy with “No-Touch” Technique:
- Standard treatment for localized, non-invasive lesions
- Wide surgical margins (≥4 mm) are recommended
- Double freeze-thaw cryotherapy applied to lesion margins
Complications: Scarring, recurrence, limbal stem cell deficiency
Topical Chemotherapy
Non-invasive or multifocal lesions may respond well to topical agents:
- Mitomycin C (MMC):
- Antimetabolite used in cycles (0.02%–0.04%)
- Requires punctal occlusion and lubrication
- 5-Fluorouracil (5-FU):
- Pyrimidine analog applied in short cycles (1% concentration)
- Minimal systemic absorption
- Interferon Alpha-2b (IFN α2b):
- Administered topically (1 MIU/ml) or via subconjunctival injection
- Fewer side effects; preferred in immunocompromised patients
Radiotherapy and Cryotherapy
Reserved for recurrent, large, or non-resectable lesions:
- Plaque brachytherapy using Sr-90
- Cryotherapy applied adjunctively with surgical excision
Follow-Up and Monitoring
Recurrence rates range from 5% to 33% depending on treatment modality and margin status. Long-term surveillance is essential:
- Quarterly exams for the first year
- Annual exams thereafter for high-risk patients
- Use of impression cytology or AS-OCT to detect subclinical recurrence
Prognosis and Outcomes
OSSN generally has a favorable prognosis when diagnosed early and treated effectively. Invasive SCC carries a higher risk of complications, including orbital invasion and metastasis, although rare.
Prognostic Factors:
- Positive surgical margins
- Immunosuppression (e.g., HIV)
- Delayed treatment
- Higher-grade histology
With multidisciplinary management, the majority of patients achieve complete remission.
Preventive Measures
Proactive steps can reduce the risk of developing OSSN, particularly in high-risk populations:
- UV protection: Sunglasses, wide-brimmed hats
- HPV vaccination in youth may reduce OSSN incidence
- HIV screening and ART adherence in HIV-positive individuals
- Avoidance of ocular surface irritants, such as chemical exposure
- Routine eye examinations for early detection
Frequently Asked Questions:
Q1: Is OSSN life-threatening?
While OSSN is typically localized and slow-growing, invasive cases can cause serious ocular complications and rarely metastasize.
Q2: Can OSSN recur after treatment?
Yes, especially if surgical margins are positive or in cases of immunosuppression. Lifelong monitoring is advised.
Q3: How is OSSN different from pterygium?
OSSN presents as a vascularized, irregular lesion with keratinization, while pterygium typically appears triangular and smooth without epithelial thickening.
Q4: Are there any lifestyle changes that help prevent OSSN?
Yes, limiting sun exposure, avoiding eye trauma or irritants, and treating chronic inflammation can reduce risk.
Q5: Is OSSN contagious?
No, OSSN is not contagious. It is a result of genetic, environmental, and viral interactions.
Ocular Surface Squamous Neoplasia is a potentially vision-threatening condition that demands early recognition and a strategic, patient-specific treatment approach. With advancements in diagnostic imaging and topical therapies, the management of OSSN has shifted toward less invasive, highly effective solutions. Collaborative care between ophthalmologists, oncologists, and pathologists ensures optimal outcomes and long-term ocular health.