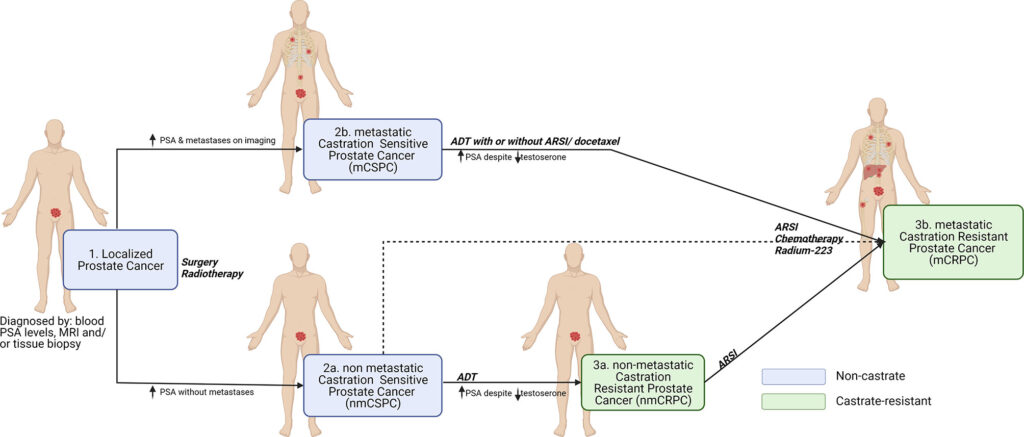
Metastatic castration-sensitive prostate cancer (mCSPC) is an advanced stage of prostate cancer where cancer cells have spread beyond the prostate gland to other parts of the body, such as bones, lymph nodes, or visceral organs. Unlike castration-resistant prostate cancer, mCSPC still responds to androgen deprivation therapy (ADT), which lowers testosterone levels to slow disease progression.
Causes and Risk Factors of mCSPC
Prostate cancer originates in the prostate gland and can metastasize when cancerous cells break away from the primary tumor and spread through the bloodstream or lymphatic system. Risk factors include:
- Age: Men over 50 are at higher risk.
- Genetics: Family history increases susceptibility.
- Hormonal Influence: Higher testosterone levels can promote cancer growth.
- Diet and Lifestyle: High-fat diets and sedentary lifestyles may contribute.
- Ethnicity: African American men have a higher incidence and mortality rate.
Symptoms of Metastatic Castration-Sensitive Prostate Cancer
While early-stage prostate cancer may be asymptomatic, metastatic progression can lead to:
- Bone pain, especially in the hips, spine, and ribs
- Fatigue and weakness
- Weight loss
- Difficulty urinating or blood in urine
- Swelling in the legs due to lymphatic obstruction
Diagnosis of mCSPC
1. Prostate-Specific Antigen (PSA) Test
A blood test measuring PSA levels is often the first step. Elevated PSA may indicate cancer progression.
2. Imaging Tests
- MRI and CT scans assess tumor spread.
- Bone scans detect bone metastases.
- PET scans provide detailed insights into cancer location.
3. Biopsy and Genetic Testing
A biopsy confirms cancer presence, while genetic testing identifies mutations such as BRCA1, BRCA2, and ATM, which may influence treatment decisions.
Treatment Options for Metastatic Castration-Sensitive Prostate Cancer
1. Androgen Deprivation Therapy (ADT)
ADT remains the cornerstone of treatment by reducing testosterone levels. Common approaches include:
- Luteinizing Hormone-Releasing Hormone (LHRH) Agonists: Leuprolide, Goserelin
- LHRH Antagonists: Degarelix
- Orchiectomy: Surgical removal of testicles to lower testosterone
2. Androgen Receptor Inhibitors
Advanced hormone therapy drugs such as enzalutamide and apalutamide block androgen receptors, reducing cancer growth.
3. Chemotherapy
Docetaxel and cabazitaxel are commonly used for patients with extensive disease progression.
4. Targeted Therapy and Immunotherapy
- PARP inhibitors (e.g., olaparib) for patients with BRCA mutations
- Checkpoint inhibitors like pembrolizumab for specific genetic profiles
5. Radiation Therapy
External beam radiation is used to control localized metastatic sites, especially for bone metastases.
6. Bone-Directed Therapy
Drugs like zoledronic acid and denosumab prevent bone loss and fractures in patients with bone metastases.
Prognosis and Survival Rates
The prognosis for mCSPC varies based on factors such as overall health, PSA levels, and response to treatment. With modern therapies, many patients experience prolonged survival and improved quality of life.
Survival Rate Estimate:
- With ADT alone: Median survival ~3 years
- With ADT + docetaxel: Median survival ~5 years
- With ADT + novel hormonal therapy: Improved survival beyond 5 years
Future Research and Clinical Trials
Ongoing clinical trials are exploring new drug combinations, immunotherapies, and genetic-based treatments to improve survival rates. Patients are encouraged to consider clinical trials for access to innovative therapies.
Metastatic castration-sensitive prostate cancer is a serious but manageable condition with the right treatment approach. Early diagnosis, personalized treatment plans, and emerging therapies continue to enhance survival and quality of life for patients.