Malignant melanoma is an aggressive form of skin cancer originating from melanocytes. Genetic mutations play a critical role in melanoma progression, with the BRAF V600K mutation being a significant subtype. This mutation affects the BRAF gene, leading to uncontrolled cell growth and increased tumor aggression. Understanding its impact, available treatments, and advancements in targeted therapy is crucial for improving patient outcomes.
BRAF V600K Mutation: An Overview
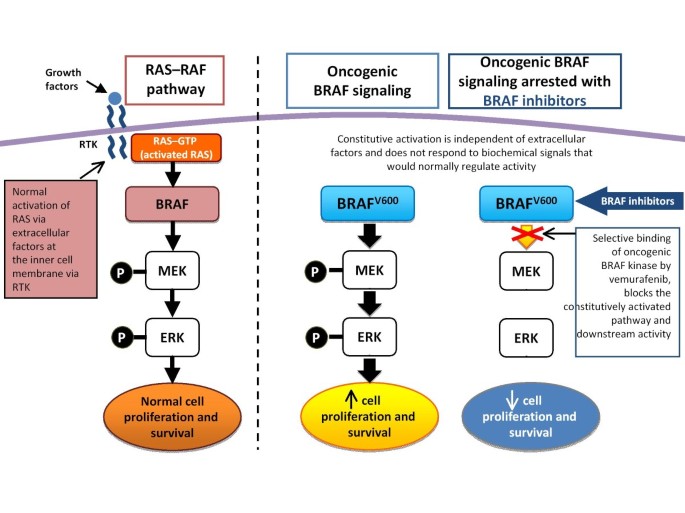
The BRAF gene encodes a protein involved in the MAPK/ERK signaling pathway, regulating cell growth and division. The V600K mutation results from a substitution of valine (V) with lysine (K) at codon 600, leading to abnormal signaling and increased tumor proliferation.
Key Characteristics of BRAF V600K Mutation
- Accounts for approximately 10-30% of BRAF-mutated melanomas.
- Associated with increased metastatic potential and higher tumor burden.
- Often found in older patients with chronic sun exposure.
- Less responsive to BRAF inhibitors alone, requiring combination therapies.
Diagnosis and Genetic Testing
Accurate diagnosis of melanoma with BRAF V600K mutation involves:
- Histopathological Examination – Identifying atypical melanocytes in biopsy samples.
- Molecular Testing – Using techniques like polymerase chain reaction (PCR) or next-generation sequencing (NGS) to detect BRAF mutations.
- Immunohistochemistry (IHC) – Differentiating BRAF-mutant and wild-type melanomas.
Treatment Strategies for BRAF V600K Melanoma
Due to the aggressive nature of BRAF V600K melanomas, treatment requires a multimodal approach.
1. Targeted Therapy
BRAF inhibitors, while effective for V600E mutations, show limited efficacy in V600K cases. Therefore, a combination approach is preferred:
- BRAF Inhibitors (e.g., Dabrafenib) – Directly inhibit mutated BRAF protein.
- MEK Inhibitors (e.g., Trametinib) – Block the downstream signaling pathway, improving response rates.
- Combination Therapy – Using both BRAF and MEK inhibitors has shown better results than monotherapy.
2. Immunotherapy
Immune checkpoint inhibitors have transformed melanoma treatment, particularly for BRAF V600K mutations:
- PD-1 Inhibitors (e.g., Pembrolizumab, Nivolumab) – Enhance the immune system’s ability to target cancer cells.
- CTLA-4 Inhibitors (e.g., Ipilimumab) – Improve long-term survival in metastatic cases.
- Combination Immunotherapy – Dual blockade therapy (PD-1 + CTLA-4) provides superior outcomes in advanced melanoma.
3. Chemotherapy
Though less effective than targeted therapy or immunotherapy, chemotherapy (e.g., dacarbazine) may be used in refractory cases.
Prognosis and Survival Rates
The prognosis for BRAF V600K melanoma varies based on stage and response to treatment:
- Localized Stage: High 5-year survival rate (>90%) with early intervention.
- Regional Spread: Moderate prognosis with aggressive treatment.
- Metastatic Stage: Lower survival rates (~20-30%) but improving with novel therapies.
Future Directions and Research
Recent advancements in melanoma research focus on:
- Next-generation BRAF inhibitors with improved selectivity.
- Personalized medicine approaches using gene expression profiling.
- Adoptive T-cell therapy and vaccine-based immunotherapy.
Malignant melanoma with BRAF V600K mutation presents unique challenges due to its aggressive nature and reduced response to traditional BRAF inhibitors. However, advancements in targeted therapy, immunotherapy, and precision medicine are improving outcomes. Early detection and personalized treatment plans remain crucial in managing this high-risk melanoma subtype.