Malignant melanoma with BRAF V600 mutation is an aggressive form of skin cancer characterized by a specific genetic alteration in the BRAF gene, leading to uncontrolled cell growth. This mutation is present in approximately 50% of melanomas and significantly influences treatment options. Advances in targeted therapy and immunotherapy have improved patient outcomes, making early detection and precise diagnosis essential.
The Role of BRAF V600 Mutation in Melanoma
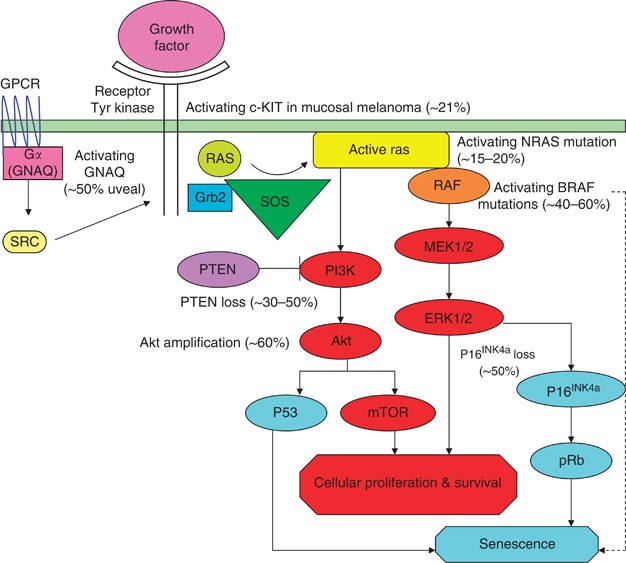
BRAF is a gene encoding a serine/threonine-protein kinase, which is crucial for the MAPK/ERK signaling pathway. The V600 mutation results in the substitution of valine (V) with glutamic acid (E) at position 600, leading to constitutive activation of the BRAF kinase, promoting cancer cell proliferation.
Types of BRAF V600 Mutations
- BRAF V600E: Most common (80–90% of cases), highly responsive to BRAF inhibitors.
- BRAF V600K: Less frequent (10–20%), more aggressive, associated with poorer prognosis.
- Rare Variants (V600R, V600D): Less studied but impact treatment responses.
Symptoms of Malignant Melanoma with BRAF V600 Mutation
Melanomas with BRAF V600 mutations exhibit typical signs of malignant melanoma:
- Rapidly growing, asymmetrical lesions
- Irregular, blurred, or uneven borders
- Multiple colors within a single mole
- Diameter larger than 6mm
- Itching, bleeding, or ulceration
- Metastatic spread to lymph nodes, lungs, brain, or liver
Diagnosis and Detection of BRAF V600 Mutation
Dermatological Examination
- Dermoscopy: Identifies suspicious lesions.
- Total-body skin photography: Tracks mole changes.
Biopsy and Pathology Tests
- Excisional biopsy: Preferred for primary melanoma.
- Immunohistochemistry (IHC): Identifies BRAF expression.
- PCR and Next-Generation Sequencing (NGS): Confirms BRAF mutation subtype.
Imaging for Staging
- CT scans and MRI: Detect metastasis.
- PET scans: Assess systemic spread.
Treatment Strategies for BRAF V600-Mutant Melanoma
Targeted Therapy: BRAF and MEK Inhibitors
BRAF inhibitors block the mutated BRAF protein, while MEK inhibitors prevent downstream signaling, enhancing treatment efficacy and reducing resistance.
Approved BRAF/MEK Inhibitor Combinations
- Dabrafenib + Trametinib
- Vemurafenib + Cobimetinib
- Encorafenib + Binimetinib
Immunotherapy Approaches
- Checkpoint Inhibitors:
- PD-1 Inhibitors: Pembrolizumab, Nivolumab
- CTLA-4 Inhibitor: Ipilimumab
- Combining immunotherapy with targeted therapy improves response rates.
Surgical and Radiation Interventions
- Surgical excision is crucial for localized tumors.
- Radiation therapy may be used for brain metastases.
Prognosis and Survival Rates
- Stage I-II: 5-year survival rate of 80–90%.
- Stage III: 50–70% survival rate.
- Stage IV (Metastatic Melanoma): Survival rates vary but have improved significantly with modern therapies.
Prevention and Future Research
- Avoid excessive UV exposure and use broad-spectrum sunscreen.
- Genetic testing for early intervention.
- Emerging therapies like mRNA vaccines and new immunotherapy agents hold promise for future treatments.
Malignant melanoma with BRAF V600 mutation represents a highly aggressive but treatable form of skin cancer. Advances in targeted therapy, immunotherapy, and combination treatments have significantly improved survival rates. Early detection through regular skin exams and genetic testing remains the most effective strategy in combating this disease.

