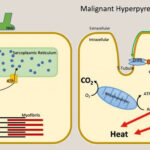
Malignant hyperthermia (MH) is a rare but life-threatening condition triggered by certain anesthetic agents and succinylcholine, leading to rapid hypermetabolism in skeletal muscles. It primarily affects individuals with a genetic predisposition.
Risk Factors for Malignant Hyperthermia
Genetic Predisposition
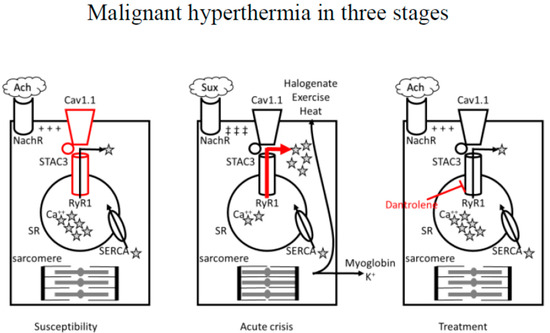
MH is inherited in an autosomal dominant manner, meaning a single defective gene from either parent can cause susceptibility. The most common genetic mutations occur in the RYR1 and CACNA1S genes.
Triggers
- Volatile anesthetics such as sevoflurane, desflurane, and halothane
- Succinylcholine, a depolarizing muscle relaxant
- High environmental temperatures and exertion in rare cases
Key Strategies for Prevention
1. Preoperative Screening and Risk Assessment
A thorough patient history is essential to identify individuals at risk. Key indicators include:
- Family history of MH or unexplained anesthesia complications
- Personal history of heat-related illness or unexplained muscle issues
2. Genetic Testing for Susceptibility
Genetic screening for RYR1 and CACNA1S mutations helps confirm susceptibility. If genetic testing is inconclusive, a caffeine-halothane contracture test (CHCT) may be performed on muscle biopsy samples.
3. Anesthesia Protocol Adjustments
For MH-susceptible patients, anesthesia protocols should include:
- Avoiding trigger agents (volatile anesthetics and succinylcholine)
- Using total intravenous anesthesia (TIVA) with non-triggering agents such as propofol
- Ensuring a clean anesthesia workstation by flushing vaporizers and circuits with fresh gas
- Keeping dantrolene readily available in case of an MH episode
4. Dantrolene Prophylaxis
Dantrolene, a muscle relaxant that inhibits calcium release in skeletal muscle, is the only FDA-approved treatment for MH. While it is mainly used during an MH crisis, some cases may warrant prophylactic administration.
5. Perioperative Temperature Monitoring
Continuous temperature monitoring during surgery allows early detection of hyperthermia. Rectal, esophageal, or core temperature probes should be used in at-risk patients.
6. Emergency Preparedness and MH Protocols
Every surgical facility should have an MH emergency cart equipped with:
- Dantrolene (minimum of 36 vials for an adult patient)
- Sodium bicarbonate to correct metabolic acidosis
- Mannitol and furosemide for renal protection
- Cooling measures such as ice packs and cold saline
Postoperative Care and Patient Education
Patients susceptible to MH should be informed about their condition and given a medical alert bracelet. They should also provide documentation of their MH status to future healthcare providers.
Preventing malignant hyperthermia requires a proactive approach involving preoperative screening, genetic testing, anesthesia modifications, and emergency preparedness. By implementing these strategies, healthcare providers can significantly reduce the risk of an MH crisis and ensure patient safety during surgical procedures.