Lymphomatous meningitis (LM), also known as leptomeningeal lymphoma, is a rare but severe complication of systemic or primary central nervous system (CNS) lymphoma. It occurs when malignant lymphocytes infiltrate the meninges, leading to neurological dysfunction. Early recognition and treatment are critical to improving patient outcomes.
Causes and Pathophysiology
LM results from the hematogenous or direct spread of lymphoma cells into the cerebrospinal fluid (CSF) and leptomeninges. The condition is most commonly associated with:
- Non-Hodgkin’s lymphoma (NHL), especially diffuse large B-cell lymphoma (DLBCL)
- Primary CNS lymphoma (PCNSL)
- Chronic lymphocytic leukemia (CLL) with CNS involvement
- Burkitt lymphoma and other aggressive subtypes
The presence of malignant lymphocytes in the CSF leads to inflammation, increased intracranial pressure, and neurological deficits.
Symptoms of Lymphomatous Meningitis
Symptoms depend on the location and extent of CNS involvement and typically include:
- Headache and nausea due to increased CSF pressure
- Cranial nerve palsies causing vision changes, facial numbness, or dysphagia
- Cognitive and behavioral changes such as confusion, memory loss, and altered mental status
- Seizures in cases of cortical involvement
- Weakness, sensory deficits, or ataxia indicating spinal cord involvement
Diagnosis
Timely diagnosis requires a combination of clinical evaluation, imaging, and laboratory tests:
- Lumbar Puncture (CSF Analysis) – Elevated protein, decreased glucose, lymphocytic pleocytosis, and detection of malignant cells via cytology or flow cytometry
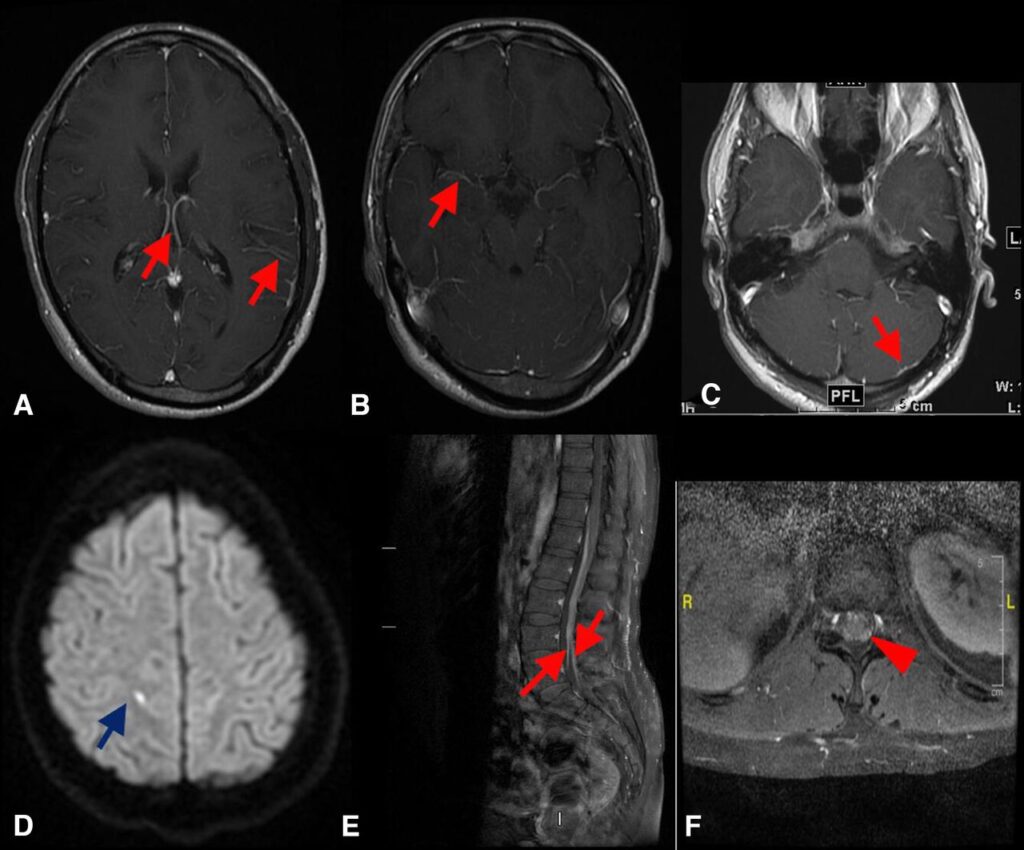
- Magnetic Resonance Imaging (MRI) with Contrast – Shows leptomeningeal enhancement, hydrocephalus, or nodular deposits
- CSF Biomarkers – Immunoglobulin gene rearrangement, MYD88 mutation in PCNSL, and cytokine profiling
- Positron Emission Tomography (PET-CT) – Assesses systemic disease burden
Treatment Options
Treatment aims to control CNS disease, alleviate symptoms, and improve survival.
Chemotherapy
- Intrathecal Chemotherapy (ITC) – Methotrexate, cytarabine, and thiotepa administered via lumbar puncture or Ommaya reservoir
- High-dose Systemic Chemotherapy – High-dose methotrexate or rituximab-based regimens for systemic disease control
Radiation Therapy
- Whole-brain or focal radiation to target meningeal involvement and reduce tumor burden
Supportive Care
- Corticosteroids (Dexamethasone) to reduce inflammation and intracranial pressure
- Antiepileptic drugs for seizure management
- CSF shunting procedures for hydrocephalus relief
Prognosis and Survival
The prognosis of LM remains poor, with a median survival of 4–6 months despite aggressive treatment. Early intervention, combined modality therapy, and novel targeted treatments may improve outcomes.
Prevention Strategies
- Regular monitoring in high-risk lymphoma patients
- Early initiation of CNS prophylaxis in aggressive lymphomas
- Routine imaging and CSF analysis for early detection
Lymphomatous meningitis is a life-threatening complication of lymphoma requiring prompt diagnosis and treatment. Advances in targeted therapy and personalized medicine offer hope for improved patient survival.

