Low-grade gliomas (LGGs) are slow-growing primary brain tumors that arise from glial cells. Among the genetic alterations associated with LGGs, the BRAF V600E mutation is a critical factor influencing tumor behavior, prognosis, and treatment response. This article explores the pathophysiology, clinical implications, and management strategies for LGGs harboring this mutation.
Understanding the BRAF V600E Mutation
The BRAF gene encodes a protein kinase that plays a crucial role in the mitogen-activated protein kinase (MAPK) pathway, which regulates cell growth and division. The V600E mutation leads to uncontrolled activation of this pathway, promoting tumor proliferation.
Epidemiology and Risk Factors
- Incidence: BRAF V600E mutations are detected in 5-10% of pediatric and adult LGGs.
- Age Group: More common in children and young adults.
- Tumor Types Associated:
- Pleomorphic xanthoastrocytoma (PXA)
- Ganglioglioma
- Pilocytic astrocytoma
- Diffuse gliomas
Clinical Presentation
Symptoms of low-grade gliomas with BRAF V600E mutation vary based on tumor location and size. Common symptoms include:
- Seizures (most frequent symptom)
- Headaches
- Cognitive impairment
- Focal neurological deficits (e.g., weakness, speech difficulties)
Diagnosis and Molecular Testing
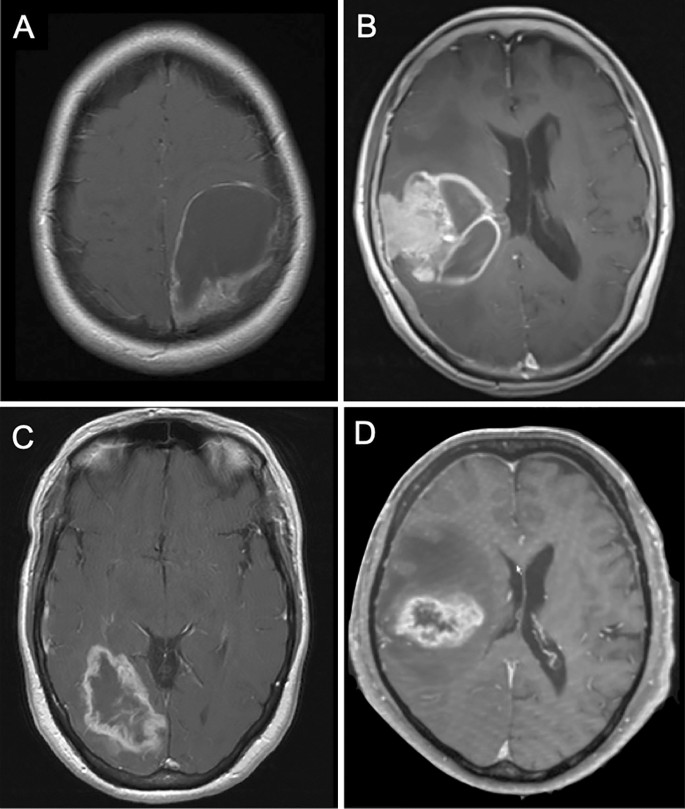
Imaging Modalities
- Magnetic Resonance Imaging (MRI):
- T2-weighted hyperintense lesion
- No significant contrast enhancement
- Positron Emission Tomography (PET): May help differentiate between low- and high-grade tumors.
Molecular and Genetic Testing
- Polymerase Chain Reaction (PCR) or Next-Generation Sequencing (NGS): Confirms the presence of BRAF V600E mutation.
- Immunohistochemistry (IHC): Detects mutant BRAF protein expression.
Prognosis and Impact of BRAF V600E Mutation
- Prognostic Implications: Tumors with this mutation tend to have a higher recurrence rate.
- Survival Rates: Generally favorable, but outcomes depend on early detection and treatment choice.
- Risk of Malignant Transformation: Higher risk of progression to high-grade glioma (e.g., glioblastoma).
Treatment Strategies
1. Surgical Resection
- Extent of Resection: Maximal safe resection improves survival.
- Challenges: Location in eloquent brain regions may limit complete removal.
2. Targeted Therapy
- BRAF Inhibitors:
- Dabrafenib and vemurafenib target the V600E mutation.
- Improved progression-free survival (PFS) in clinical trials.
- MEK Inhibitors:
- Trametinib and cobimetinib block downstream signaling.
- Effective in combination therapy.
3. Radiation Therapy
- Indications: Used in residual or recurrent tumors.
- Risk Considerations: Potential neurocognitive decline in young patients.
4. Chemotherapy
- Temozolomide (TMZ): Commonly used, but response varies.
- Carboplatin/Vincristine: Used in pediatric patients.
Emerging Research and Clinical Trials
- Ongoing studies are evaluating novel BRAF/MEK inhibitor combinations.
- Immunotherapy approaches are under investigation for improved outcomes.
- Liquid biopsy techniques are being explored for non-invasive tumor monitoring.
Low-grade gliomas with BRAF V600E mutation represent a distinct molecular subgroup with unique treatment considerations. Advancements in targeted therapy and precision medicine continue to improve patient outcomes. Early diagnosis and personalized treatment plans remain crucial for optimizing prognosis.

