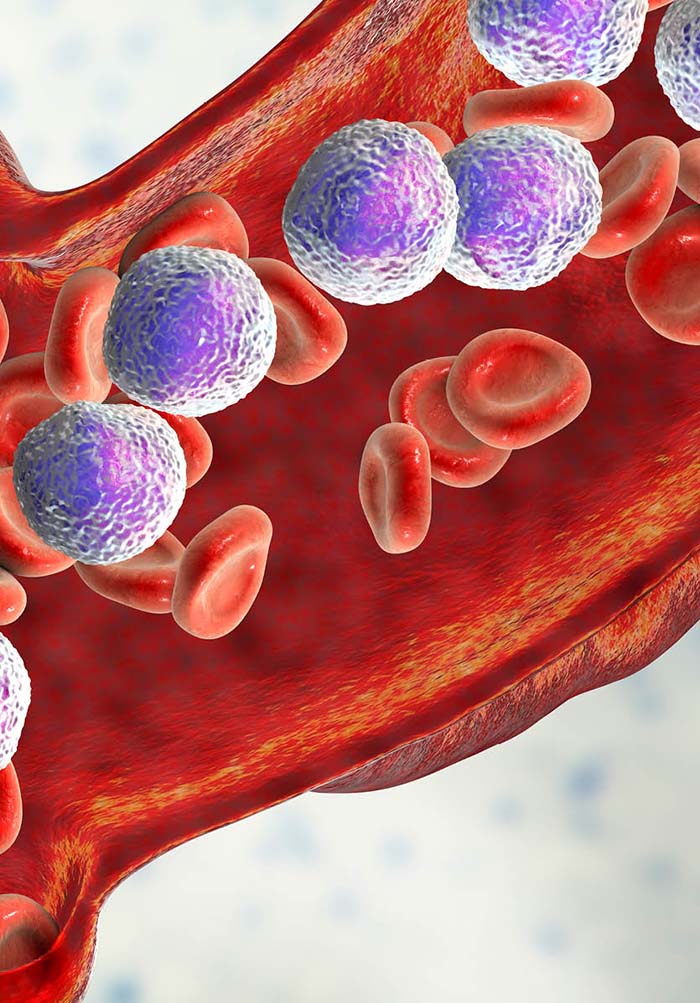
Juvenile Myelomonocytic Leukemia (JMML) is a rare and aggressive form of childhood leukemia that affects young children, primarily those under the age of four. It originates in the bone marrow and leads to the overproduction of myelomonocytic white blood cells, which crowd out normal blood cells and disrupt immune function. Unlike acute leukemias, JMML is classified as a mixed myelodysplastic/myeloproliferative disorder (MDS/MPD), making it distinct in its progression and treatment.
Causes and Risk Factors of JMML
JMML is primarily associated with genetic mutations rather than external environmental factors. The most common mutations linked to JMML include:
- RAS Pathway Mutations: Found in over 90% of cases, these affect genes such as NRAS, KRAS, PTPN11, and CBL.
- Neurofibromatosis Type 1 (NF1): A genetic disorder that significantly increases the risk of JMML.
- Germline Mutations: Some cases arise due to inherited mutations, particularly in CBL and RAS genes.
- Epigenetic Abnormalities: Aberrant DNA methylation patterns have been linked to disease severity and prognosis.
Symptoms of JMML
JMML symptoms often develop gradually and can be mistaken for other illnesses. The most common signs include:
- Persistent Fever – Unexplained high temperatures that do not subside with typical treatments.
- Pale Skin (Anemia) – Due to decreased red blood cell production.
- Enlarged Spleen and Liver (Hepatosplenomegaly) – Leads to abdominal swelling and discomfort.
- Unexplained Bruising and Bleeding – Resulting from reduced platelet levels.
- Frequent Infections – Due to an abnormal immune response.
- Skin Rash – Brownish papules caused by leukemic infiltration of the skin.
- Failure to Thrive – Poor weight gain and developmental delays in infants.
How is JMML Diagnosed?
JMML diagnosis requires a combination of laboratory tests and genetic analysis:
- Complete Blood Count (CBC) and Peripheral Blood Smear: Shows elevated monocyte counts and low platelet levels.
- Bone Marrow Aspiration and Biopsy: Confirms the presence of abnormal myelomonocytic cells.
- Genetic Testing: Identifies mutations in NRAS, KRAS, PTPN11, CBL, or NF1 genes.
- Molecular and Cytogenetic Analysis: Helps determine disease severity and prognosis.
- Fetal Hemoglobin (HbF) Levels: Elevated HbF levels are often associated with JMML.
Treatment Options for JMML
JMML treatment is challenging due to its aggressive nature. The main treatment options include:
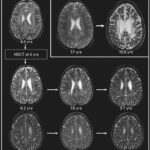
1. Hematopoietic Stem Cell Transplantation (HSCT)
- The only curative treatment for JMML.
- Success rates vary between 50-60%, depending on donor compatibility and disease status.
- Some patients may require a second transplant if the disease recurs.
2. Chemotherapy
- Used primarily as a bridge therapy before HSCT.
- Low-dose chemotherapy (e.g., cytarabine, azacitidine) helps reduce leukemic burden.
3. Targeted Therapy
- Experimental treatments focus on RAS pathway inhibitors like MEK inhibitors (trametinib, selumetinib).
- FLT3 inhibitors and hypomethylating agents (azacitidine, decitabine) show promise in clinical trials.
4. Supportive Care
- Blood transfusions to manage anemia.
- Antibiotics to prevent infections.
- Splenectomy in rare cases where spleen enlargement is severe.
Prognosis and Survival Rates
JMML prognosis depends on several factors:
- Genetic Profile: Patients with PTPN11 mutations generally have a poorer prognosis.
- Age at Diagnosis: Children diagnosed before age two have a better survival rate.
- Treatment Response: A successful bone marrow transplant significantly improves survival.
- Relapse Rates: Disease recurrence occurs in approximately 30-40% of cases post-HSCT.
The 5-year survival rate for JMML patients who receive a successful stem cell transplant is around 50-60%. However, without treatment, JMML is almost always fatal within a few years of diagnosis.
Ongoing Research and Future Perspectives
Current research focuses on:
- New RAS pathway inhibitors for targeted treatment.
- Immunotherapy approaches such as CAR-T cell therapy.
- Advanced genetic profiling to identify high-risk patients early.
- Combination therapies to improve HSCT outcomes.
Juvenile Myelomonocytic Leukemia (JMML) is a rare yet aggressive childhood leukemia with a complex genetic basis. Early diagnosis, genetic testing, and hematopoietic stem cell transplantation are critical for improving survival rates. Ongoing research into targeted therapies offers hope for better treatment outcomes in the future.