An intra-abdominal Peptococcus abscess is a localized collection of pus caused by an infection with Peptococcus bacteria, a genus of anaerobic, Gram-positive cocci. While Peptococcus species are part of the normal flora of the gastrointestinal tract, they can become pathogenic under certain conditions, leading to severe infections. Early recognition and management are crucial to prevent complications such as sepsis and organ failure.
Causes and Risk Factors
Peptococcus infections typically occur in polymicrobial settings alongside other anaerobic and facultative bacteria. The most common causes include:
- Perforation of the Gastrointestinal Tract: Due to conditions like appendicitis, diverticulitis, or peptic ulcers.
- Post-Surgical Infections: Following abdominal surgeries such as bowel resections or perforation repairs.
- Trauma: Penetrating abdominal injuries can introduce bacteria into normally sterile areas.
- Intra-Abdominal Malignancies: Cancers may cause necrosis, leading to abscess formation.
- Immunosuppression: Conditions like diabetes, HIV, or prolonged steroid use increase susceptibility.
Symptoms and Clinical Presentation
The symptoms of an intra-abdominal Peptococcus abscess can vary but typically include:
- Persistent abdominal pain and tenderness
- Fever and chills, indicating systemic infection
- Nausea and vomiting, often leading to dehydration
- Localized swelling or a palpable mass
- Changes in bowel movements, such as diarrhea or constipation
- Sepsis symptoms, including hypotension and tachycardia in severe cases
Diagnosis
A thorough clinical evaluation, imaging, and laboratory tests are necessary for an accurate diagnosis. The key diagnostic steps include:
1. Laboratory Tests
- Complete Blood Count (CBC): Shows elevated white blood cells (WBC) due to infection.
- Blood Cultures: May detect bacteremia in severe cases.
- Inflammatory Markers: Elevated C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR) suggest infection.
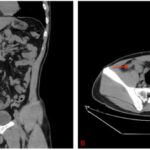
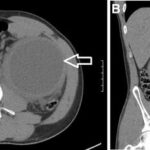
2. Imaging Studies
- Ultrasound: Useful for initial assessment of abscesses.
- Computed Tomography (CT) Scan: The gold standard for detecting intra-abdominal abscesses, determining their size, and guiding drainage.
- Magnetic Resonance Imaging (MRI): Occasionally used for complex cases.
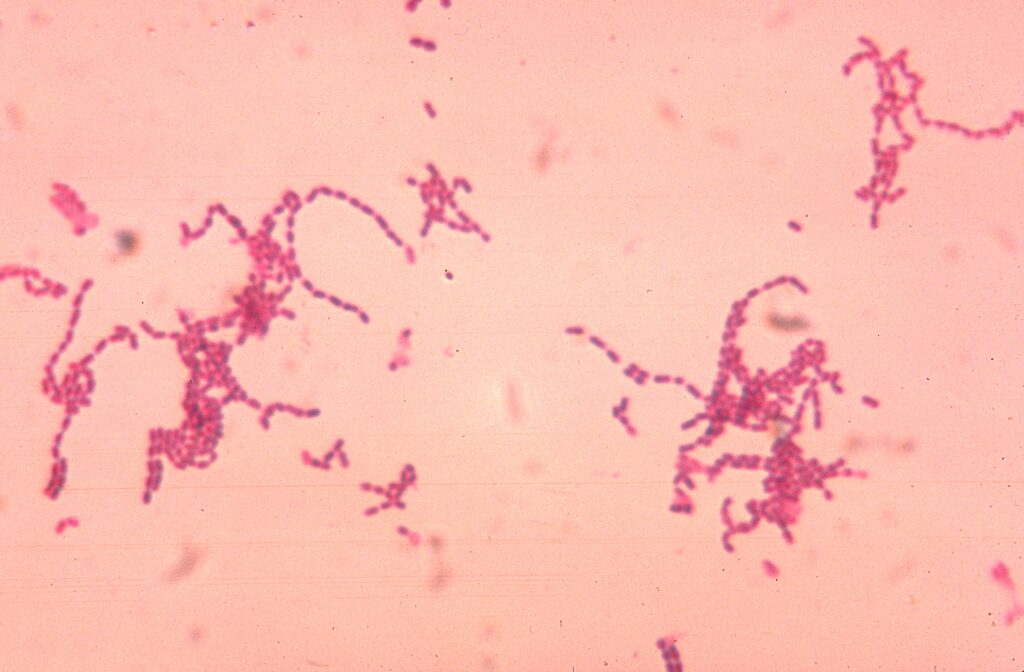
3. Microbiological Analysis
- Abscess Aspiration and Culture: Identifies the causative bacteria and helps tailor antibiotic therapy.
- Gram Stain and Anaerobic Culture: Confirms the presence of Peptococcus species.
Treatment Strategies
Management of intra-abdominal Peptococcus abscess requires a combination of antibiotic therapy and surgical or percutaneous drainage.
1. Antibiotic Therapy
- Empirical broad-spectrum antibiotics covering anaerobes and facultative bacteria:
- Metronidazole (for anaerobes) + Piperacillin-tazobactam or Carbapenems
- Clindamycin as an alternative in penicillin-allergic patients
- Targeted therapy based on culture results
- Duration: Typically 4–6 weeks, adjusted based on clinical response
2. Surgical and Percutaneous Drainage
- Percutaneous Drainage (PCD): Preferred for well-localized abscesses and performed under ultrasound or CT guidance.
- Surgical Drainage: Required for larger, complex, or multi-loculated abscesses.
- Laparoscopic vs. Open Surgery: Laparoscopic drainage offers faster recovery, while open surgery is reserved for severe cases.
3. Supportive Care
- Intravenous fluids to maintain hydration
- Pain management with non-opioid or opioid analgesics
- Nutritional support, including enteral or parenteral feeding if needed
Complications
If left untreated, intra-abdominal Peptococcus abscesses can lead to:
- Sepsis and septic shock
- Peritonitis, spreading the infection across the peritoneal cavity
- Fistula formation, leading to abnormal connections between organs
- Recurrence, necessitating prolonged treatment
Prevention Strategies
- Prompt treatment of abdominal infections (e.g., appendicitis, diverticulitis)
- Sterile surgical techniques to minimize post-operative infections
- Antibiotic prophylaxis in high-risk surgical patients
- Regular follow-ups to monitor for recurrence in immunocompromised individuals
An intra-abdominal Peptococcus abscess is a serious condition requiring timely diagnosis and aggressive treatment. Early antibiotic therapy, coupled with image-guided drainage or surgical intervention, is essential to reduce morbidity and mortality. Preventive measures, including strict infection control and post-surgical monitoring, play a crucial role in minimizing the risk of abscess formation.