Gestational trophoblastic neoplasia (GTN) is a rare but serious condition characterized by abnormal growth of cells inside the uterus following conception. It falls under the broader category of gestational trophoblastic disease (GTD) and often arises after a molar pregnancy, miscarriage, or even a normal delivery.
Types of Gestational Trophoblastic Neoplasia
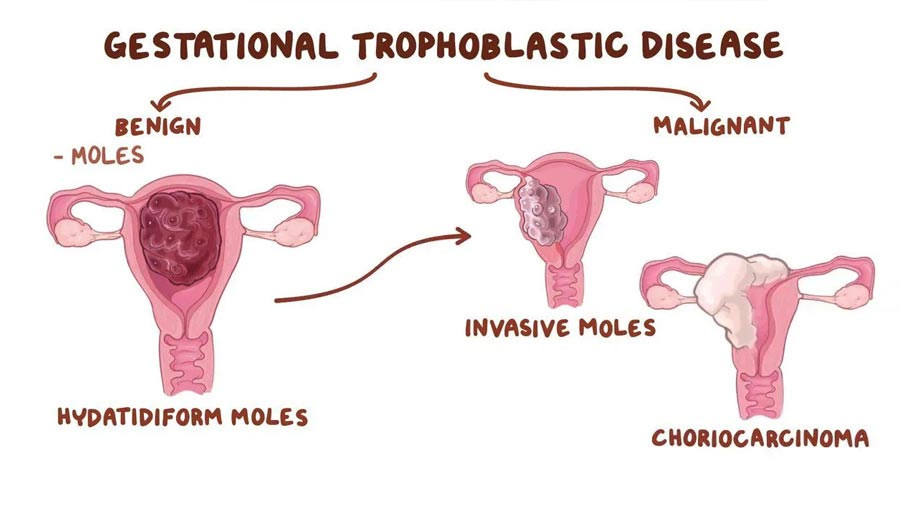
GTN comprises several malignant conditions that demand specialized treatment approaches. Key types include:
- Invasive Mole
- Develops from a hydatidiform mole (molar pregnancy) and invades the uterine wall.
- Choriocarcinoma
- A highly malignant and fast-spreading cancer often linked to previous pregnancies.
- Placental Site Trophoblastic Tumor (PSTT)
- A rare form of GTN that grows from the placental implantation site.
- Epithelioid Trophoblastic Tumor (ETT)
- A slow-growing but potentially metastatic condition that mimics PSTT.
Causes and Risk Factors
Several factors may increase the risk of developing GTN:
- Previous molar pregnancy
- Advanced maternal age (over 40)
- History of miscarriage or abortion
- Genetic predisposition
Symptoms of Gestational Trophoblastic Neoplasia
Common signs indicating GTN include:
- Abnormal vaginal bleeding (particularly post-pregnancy)
- Elevated hCG (human chorionic gonadotropin) levels
- Pelvic pain or pressure
- Enlarged uterus
- Nausea and vomiting (severe and persistent)
Diagnostic Procedures
Accurate diagnosis is essential for effective treatment. Key diagnostic methods include:
- Ultrasound: Identifies abnormal uterine masses.
- hCG Blood Tests: Tracks hormone levels to detect persistent GTN.
- Pelvic Examination: Assesses uterine size and tenderness.
- CT Scan/MRI: Identifies metastatic spread.
Treatment Options for GTN
Effective treatments are available with promising outcomes, especially when detected early. Key approaches include:
- Chemotherapy
- Primary treatment for most GTN cases.
- Drugs such as methotrexate or dactinomycin are commonly used.
- Surgery
- Recommended for resistant or localized tumors.
- Hysterectomy may be required in severe cases.
- Radiation Therapy
- Utilized for GTN that has spread beyond the uterus.
Prognosis and Recovery
GTN has a high cure rate, especially in early stages. With appropriate treatment, the prognosis is generally excellent. Regular follow-up appointments and monitoring of hCG levels are crucial for detecting recurrence.
Preventive Measures
While prevention is challenging, early detection through regular prenatal care and prompt treatment of molar pregnancies can reduce the risk of GTN.
Frequently Asked Questions
Q1: Is GTN a form of cancer?
Yes, GTN is considered a group of rare tumors that can spread if untreated. However, it responds well to treatment.
Q2: Can GTN affect future pregnancies?
Most women successfully conceive again after GTN treatment, provided hCG levels return to normal and remain stable.
Q3: How common is GTN?
GTN is rare, occurring in about 1 in 1,000 pregnancies worldwide.
Q4: What follow-up care is required after GTN treatment?
Patients typically undergo hCG monitoring for 6-12 months to ensure complete remission.
Q5: Are there lifestyle changes to support recovery?
A balanced diet, stress management, and consistent follow-up care can significantly improve recovery outcomes.