Cystinuria is a rare inherited disorder that leads to the formation of recurrent kidney stones due to excessive excretion of cystine in the urine. This condition results from a defect in amino acid transport in the kidneys, making cystine insoluble and prone to crystallization. Without proper management, it can cause severe complications, including chronic kidney disease.
Etiology and Pathophysiology
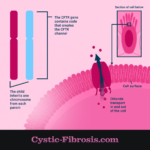
Cystinuria is caused by mutations in the SLC3A1 and SLC7A9 genes, which are responsible for encoding transporter proteins that reabsorb cystine and other dibasic amino acids (lysine, arginine, and ornithine) in the renal proximal tubules. The defective transporter allows cystine to accumulate in urine, where it forms poorly soluble crystals, leading to stone formation.
Pathophysiological Mechanism
Genetic Inheritance
Cystinuria follows an autosomal recessive inheritance pattern, meaning an individual must inherit two defective copies—one from each parent—to develop the disease. Carriers, who have only one mutated gene, typically do not exhibit symptoms but can pass the mutation to offspring.
Epidemiology
- Affects approximately 1 in 7,000 individuals worldwide.
- Both males and females are equally susceptible.
- Symptoms typically manifest in childhood or early adulthood with recurrent kidney stone episodes.
Clinical Manifestations
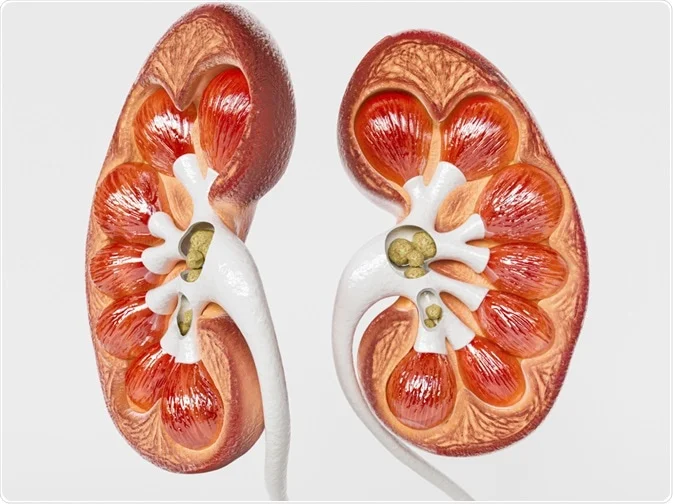
The primary symptom of cystinuria is the formation of cystine stones, leading to:
- Severe flank pain (renal colic) due to urinary tract obstruction.
- Hematuria (blood in urine) caused by irritation from passing stones.
- Frequent urinary tract infections (UTIs) due to obstructions.
- Hydronephrosis (swelling of the kidney) from stone blockage.
- Potential chronic kidney disease (CKD) with recurrent stone formation.
Diagnosis
1. Urinalysis
- Detects hexagonal cystine crystals, a characteristic sign of cystinuria.
2. Cyanide-Nitroprusside Test
- A qualitative test that turns purple in the presence of cystine, confirming excessive urinary cystine levels.
3. Imaging Studies
- CT Scan: Preferred method as cystine stones are often radiolucent on X-rays.
- Ultrasound: May help detect larger stones but is less sensitive for small ones.
4. 24-Hour Urine Collection
- Measures cystine concentration and assesses urinary pH and volume to guide treatment.
5. Genetic Testing
- Identifies mutations in SLC3A1 or SLC7A9 genes for definitive diagnosis.
Management Strategies
1. Increased Hydration
- Drinking at least 3-4 liters of water per day to dilute urine and prevent cystine crystallization.
2. Urine Alkalinization
- Potassium citrate or sodium bicarbonate is used to maintain a urine pH above 7.0, increasing cystine solubility.
3. Dietary Modifications
- Low sodium intake (<2,000 mg/day) reduces cystine excretion.
- Moderate protein restriction helps decrease cystine levels in urine.
4. Pharmacological Therapy
- Thiol-binding agents (Tiopronin, D-Penicillamine) form more soluble cystine complexes for easier excretion.
- Captopril, an ACE inhibitor, may have mild cystine-reducing effects.
5. Surgical and Minimally Invasive Procedures
- Extracorporeal Shock Wave Lithotripsy (ESWL): Not very effective for cystine stones due to their hardness.
- Ureteroscopy with Laser Lithotripsy: Used for smaller stones in the ureter.
- Percutaneous Nephrolithotomy (PCNL): Preferred for large or multiple stones.
Prognosis and Follow-Up
With early diagnosis and proper management, individuals with cystinuria can prevent frequent stone formation and protect kidney function. Lifelong monitoring, including:
- Regular urinalysis and 24-hour urine tests to assess treatment effectiveness.
- Periodic imaging studies to detect new stone formation.
- Dietary and medication adherence to prevent recurrence.