Acute promyelocytic leukemia (APL) is a distinct subtype of acute myeloid leukemia (AML), characterized by the translocation between chromosomes 15 and 17, resulting in the fusion gene PML-RARA. This genetic abnormality disrupts cell differentiation, leading to the accumulation of abnormal promyelocytes in the bone marrow and peripheral blood. APL is a medical emergency due to its high risk of life-threatening coagulopathy.
Pathophysiology of APL
APL arises from a chromosomal translocation t(15;17)(q22;q21), creating the PML-RARA fusion gene. This abnormal gene impairs myeloid cell maturation, leading to the proliferation of immature promyelocytes. A hallmark of APL is disseminated intravascular coagulation (DIC), a severe bleeding disorder resulting from the release of procoagulant molecules by malignant cells.
Clinical Presentation
Patients with APL often exhibit the following signs and symptoms:
- Easy bruising and bleeding: Due to severe coagulopathy.
- Petechiae and purpura: Small hemorrhagic spots on the skin.
- Fatigue and weakness: Resulting from anemia.
- Fever and infections: Due to neutropenia.
- Gingival bleeding and epistaxis: Common early symptoms.
Diagnosis of APL
The diagnosis of APL requires a combination of morphological, cytogenetic, and molecular analyses:
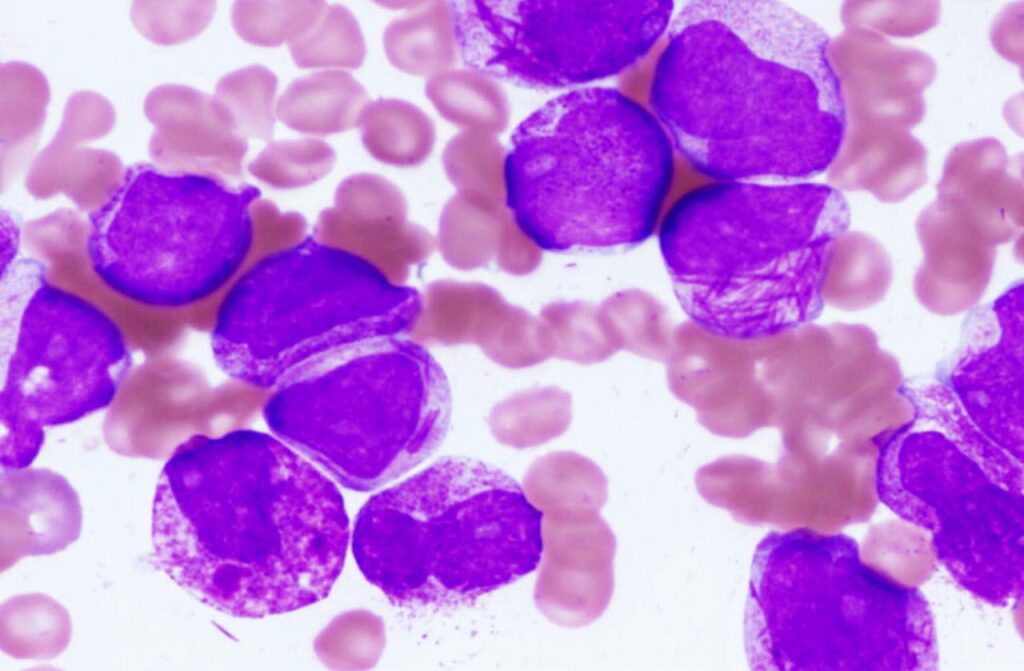
- Peripheral Blood Smear and Bone Marrow Biopsy: Reveals abnormal promyelocytes with Auer rods.
- Cytogenetics: Identifies the t(15;17) translocation.
- Polymerase Chain Reaction (PCR): Detects the PML-RARA fusion gene.
- Flow Cytometry: Confirms immunophenotypic markers characteristic of APL.
Treatment Strategies
1. All-Trans Retinoic Acid (ATRA) Therapy
ATRA, a vitamin A derivative, promotes differentiation of malignant promyelocytes into mature neutrophils, reducing disease burden and preventing coagulopathy.
2. Arsenic Trioxide (ATO) Therapy
ATO induces apoptosis in leukemia cells and is often combined with ATRA as first-line therapy, particularly in low- and intermediate-risk patients.
3. Chemotherapy (Anthracyclines)
For high-risk patients, anthracycline-based chemotherapy (e.g., idarubicin) is combined with ATRA to achieve complete remission.
4. Supportive Care
- Blood product transfusions: To manage coagulopathy.
- Antifibrinolytic agents: To control excessive bleeding.
- Infection prophylaxis: Using antibiotics and antifungal agents to prevent complications.
Prognosis and Long-Term Outcomes
With the advent of ATRA and ATO therapy, APL has become one of the most curable forms of acute leukemia. The overall survival rate exceeds 90% in patients receiving timely treatment. However, early mortality due to bleeding complications remains a concern.
Acute promyelocytic leukemia is a medical emergency requiring prompt recognition and treatment. Advances in targeted therapy have revolutionized APL management, transforming it into a highly curable disease. Early diagnosis and a structured treatment approach significantly improve patient outcomes.

