Acute Monocytic Leukemia (AML-M5) is a subtype of acute myeloid leukemia (AML) characterized by the proliferation of monoblasts and promonocytes in the bone marrow and peripheral blood. This aggressive hematologic malignancy predominantly affects adults but can also be seen in children. Understanding its pathogenesis, clinical manifestations, and treatment options is critical for improving patient outcomes.
Pathophysiology of AML-M5
AML-M5 arises from genetic mutations in hematopoietic stem cells, leading to the uncontrolled proliferation of monocytic precursors. The accumulation of immature monocytes disrupts normal hematopoiesis, resulting in cytopenias and systemic complications.
Risk Factors and Causes
Several factors contribute to the development of AML-M5:
- Genetic Mutations: FLT3, NPM1, and KMT2A rearrangements
- Prior Chemotherapy or Radiation Exposure
- Environmental Toxins: Benzene and other carcinogens
- Underlying Hematologic Disorders: Myelodysplastic syndromes
- Viral Infections: Epstein-Barr virus (EBV) and human T-cell leukemia virus (HTLV-1)
Clinical Symptoms
Patients with AML-M5 commonly present with:
- Persistent Fatigue and Weakness
- Frequent Infections and Fever
- Easy Bruising and Bleeding (Thrombocytopenia)
- Gum Hypertrophy and Gingival Infiltration
- Bone Pain and Joint Discomfort
- Leukemic Skin Infiltrates (Leukemia Cutis)
- Enlarged Liver and Spleen (Hepatosplenomegaly)
Diagnostic Evaluation
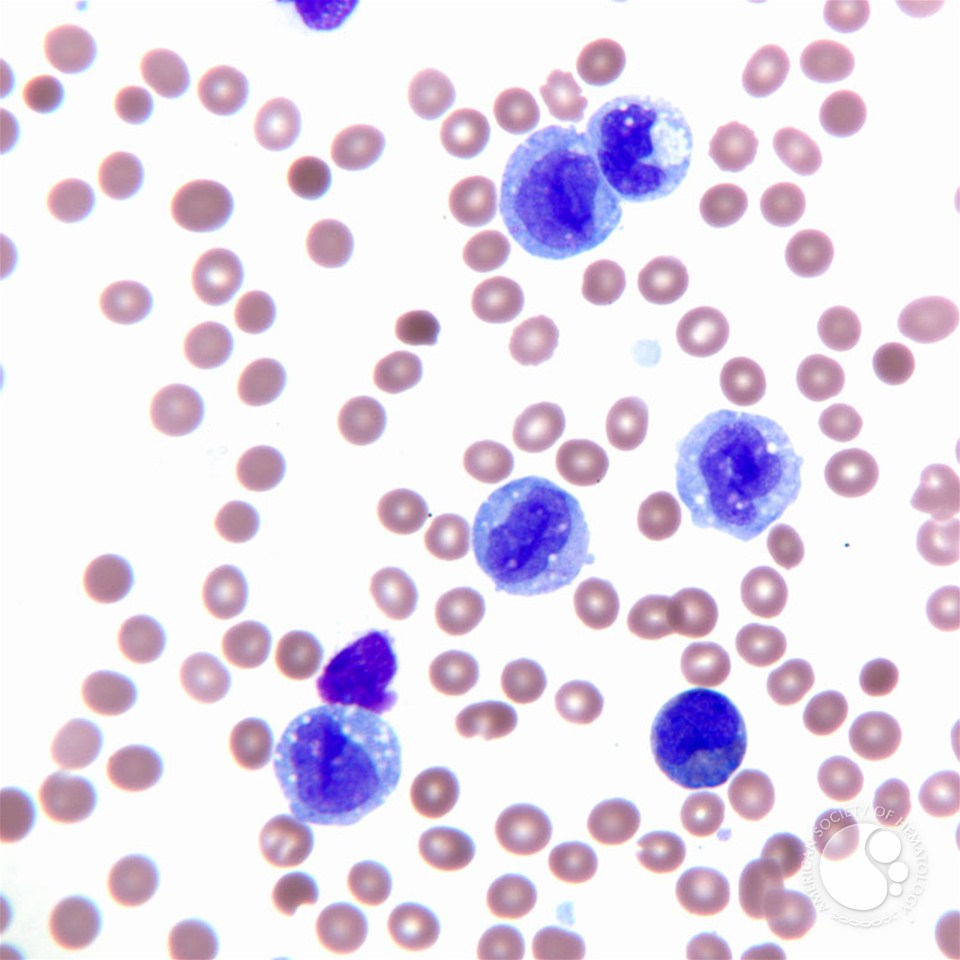
1. Complete Blood Count (CBC) and Peripheral Blood Smear
- Elevated white blood cell count with circulating monoblasts
- Anemia and thrombocytopenia
2. Bone Marrow Biopsy and Flow Cytometry
- Bone marrow biopsy reveals >80% monocytic lineage involvement
- Flow cytometry shows markers: CD14, CD64, CD11c, and CD68
3. Cytogenetic and Molecular Testing
- Karyotyping identifies chromosomal abnormalities
- Molecular testing detects FLT3, NPM1, and KMT2A mutations
4. Imaging Studies
- CT/MRI scans assess organ involvement
- Lumbar puncture evaluates central nervous system (CNS) infiltration
Treatment Strategies
1. Induction Chemotherapy
- Standard 7+3 regimen (Cytarabine + Anthracycline)
- High-risk patients may require FLT3 inhibitors (Midostaurin)
2. Consolidation Therapy
- High-dose Cytarabine (HiDAC) for younger patients
- Allogeneic stem cell transplantation (SCT) in high-risk cases
3. Targeted Therapy and Immunotherapy
- Venetoclax + Azacitidine: BCL-2 inhibition in elderly patients
- Gemtuzumab Ozogamicin (GO): Anti-CD33 therapy
- FLT3 Inhibitors: Gilteritinib and Midostaurin for FLT3-mutated AML
4. Supportive Care
- Antimicrobial Prophylaxis: To prevent infections
- Transfusion Support: Red blood cells and platelet transfusions
- Growth Factors (G-CSF): Enhances neutrophil recovery
Prognosis and Survival Rates
Prognosis depends on cytogenetic risk factors, age, and response to initial treatment. The 5-year survival rate for AML-M5 ranges from 25% to 50%, with improved outcomes in younger patients undergoing allogeneic stem cell transplantation.
Acute Monocytic Leukemia is an aggressive hematologic malignancy requiring early diagnosis and tailored therapy. Advances in molecular-targeted treatments and immunotherapy continue to improve patient survival. Future research should focus on personalized medicine to optimize treatment efficacy and reduce relapse rates.