Accelerated phase chronic myelocytic leukemia (CML) represents a critical transition in the progression of this hematologic malignancy. Proper understanding, timely diagnosis, and effective treatment strategies are vital to improving patient outcomes. This article provides an in-depth examination of accelerated phase CML, focusing on its causes, symptoms, diagnostic criteria, and treatment options.

What is Chronic Myelocytic Leukemia (CML)?
Chronic myelocytic leukemia, also known as chronic myeloid leukemia, is a type of blood cancer originating in the bone marrow. It is characterized by the overproduction of abnormal white blood cells. CML progresses through three stages:
- Chronic Phase: The earliest stage with fewer symptoms.
- Accelerated Phase: Marked by worsening disease and resistance to standard treatments.
- Blast Crisis Phase: The most severe stage, resembling acute leukemia.
The accelerated phase is a critical intermediary stage that demands immediate intervention to prevent progression to the blast crisis.
Causes and Pathophysiology of Accelerated Phase CML
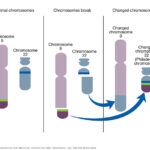
The primary cause of CML is a genetic abnormality called the Philadelphia chromosome. This results from a reciprocal translocation between chromosomes 9 and 22, creating the BCR-ABL1 fusion gene. This gene encodes a tyrosine kinase enzyme that promotes unchecked cell proliferation and inhibits apoptosis.
During the accelerated phase, genetic instability increases, leading to additional mutations and an accumulation of leukemic cells. The disease becomes more resistant to treatment, with faster progression compared to the chronic phase.
Key Factors Contributing to the Accelerated Phase
- Acquired Mutations: Further mutations in the BCR-ABL1 gene or other genetic alterations.
- Resistance to Therapy: Reduced effectiveness of tyrosine kinase inhibitors (TKIs).
- Bone Marrow Dysfunction: Increased fibrosis and impaired normal blood cell production.
Symptoms of Accelerated Phase CML
Patients in the accelerated phase may experience worsening symptoms, including:
- Fatigue: Due to anemia or decreased red blood cell production.
- Frequent Infections: Resulting from reduced functional white blood cells.
- Bleeding or Bruising: Caused by low platelet counts (thrombocytopenia).
- Weight Loss: Associated with disease progression.
- Abdominal Discomfort: Often due to an enlarged spleen (splenomegaly).
Additionally, some patients may notice symptoms from the chronic phase intensifying or new complications arising.
Diagnostic Criteria for Accelerated Phase CML
The diagnosis of the accelerated phase relies on clinical features, blood tests, and bone marrow examination. The World Health Organization (WHO) criteria for diagnosing accelerated phase CML include:
- Increased Blast Cells: 10–19% of peripheral blood or bone marrow cells are blasts.
- Basophilia: Peripheral blood basophils >20%.
- Thrombocytopenia or Thrombocytosis: Platelet counts persistently <100,000/μL or >1,000,000/μL unrelated to therapy.
- Cytogenetic Evolution: Additional chromosomal abnormalities in the Ph+ clone.
- Progressive Splenomegaly: Not responsive to therapy.
Laboratory tests such as complete blood count (CBC), cytogenetic analysis, and molecular testing for BCR-ABL1 transcripts are essential for confirmation.
Treatment Strategies for Accelerated Phase CML
Treatment during the accelerated phase aims to control disease progression, manage symptoms, and delay transformation to the blast crisis phase. A multi-modal approach is often necessary.
Tyrosine Kinase Inhibitors (TKIs)
TKIs remain the cornerstone of treatment for CML. In the accelerated phase, patients may require:
- Dose Adjustment: Higher doses of TKIs like imatinib, dasatinib, or nilotinib.
- Second-Generation TKIs: If resistance develops to first-generation TKIs, second-generation options such as bosutinib or ponatinib are effective.
Allogeneic Stem Cell Transplantation (ASCT)
ASCT is a potentially curative option, particularly for younger patients or those unresponsive to TKIs. It involves the transplantation of healthy donor stem cells after high-dose chemotherapy to eradicate leukemic cells.
Chemotherapy
For patients who are not candidates for transplantation or when disease progression is rapid, chemotherapy may help control leukemic cell proliferation.
Clinical Trials
Participation in clinical trials can provide access to novel therapies targeting specific genetic mutations or alternative pathways contributing to CML progression.
Prognosis and Monitoring
The prognosis for patients in the accelerated phase depends on the response to treatment and underlying genetic factors. Regular monitoring through:
- Quantitative PCR: Measures BCR-ABL1 transcript levels.
- Bone Marrow Biopsies: Evaluates disease progression.
- Cytogenetic Testing: Detects additional chromosomal abnormalities.
Lifestyle and Supportive Care
While medical treatments are paramount, supportive care can help manage symptoms and improve quality of life. Patients are encouraged to:
- Maintain a Healthy Diet: To support immune function and overall health.
- Engage in Light Physical Activity: To reduce fatigue and improve circulation.
- Seek Psychological Support: To cope with the emotional burden of a CML diagnosis.
Accelerated phase chronic myelocytic leukemia is a pivotal stage in the progression of CML that requires prompt and aggressive treatment. By understanding its pathophysiology, symptoms, and treatment options, healthcare professionals can tailor strategies to improve patient outcomes and delay progression to the blast crisis phase. Regular monitoring and advancements in therapy continue to enhance survival rates and quality of life for patients with accelerated phase CML.